Biomedical Engineering Reference
In-Depth Information
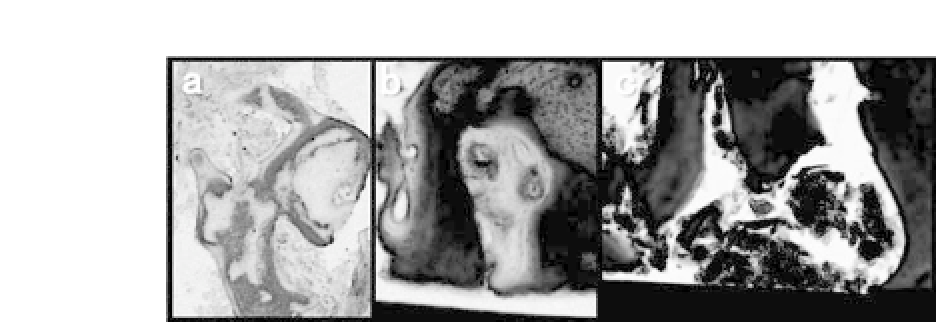
Figure 26.9.
Histology of regenerated bone. Six months after cell trans-
plantation, a bone biopsy was performed using a trephine bur at the site
of implant placement. Nondecalcified tissue sections were cut, and the sec-
tions were stained with Villanueva-Goldner stain. Newly formed bone was
observed adjacent to the scaffold, and the scaffolds seemed like they were
absorbedbyosteoclasticcells(a,b).Bonealsoformedbetweenthescaffolds.
Inthesecases,itseemedlikethescaffoldsweredegradedspontaneously(c).
See also Color Insert.
actively by osteoclastic cells since cells were not observed close to
the degrading scaffold (Fig. 26.9). Actual tissues display a combina-
tion of two types of degradation. Compared with the transplanta-
tion of bone substitute alone, the presence of new bone adjacent to
the scaffold was more frequent, which may reflect the role of trans-
planted cells. However, quantitative analyses were not performed,
and these observationsrequire further investigation.
26.3.4
Considerations for Designing Scaffolds for Clinical
Bone Tissue Engineering
Factorstoconsiderforsuccessfulscaffoldmaterialsincludebiocom-
patibility, degradation time, and mechanical properties. For bone
tissue engineering scaffolds, morphology is important. In terms of
ceramic-basedscaffolds,porousstructureisimportantandacertain
size of pore is essential for osteoconductivity, as described above.
In terms of fibrous scaffolds, fiber diameter also affects the suc-
cess of bone regeneration. Alveolar bone defects do not bear large
physiological loads until after the implant placement. Accordingly,
mechanical strength of the scaffold may not be critical for dental
implants.However,mechanicalstrengthisimportantformostortho-
pedic applications. The shape of the scaffold is also important. Bone







Search WWH ::

Custom Search