Biomedical Engineering Reference
In-Depth Information
defects in alveolar bone are small and complex in shape and so are
di
cult to treat with block-type scaffolds. On the other hand, seg-
mental bone defects may require solid, block-type scaffolds to sup-
port the mechanical strength.
The process of clinical bone tissue engineering can be divided
into at least three phases: generation of tissue grafts for transplan-
tation, scaffold degradation as bone regeneration occurs, and nor-
mal remodeling of the newly formed bone. The initial phase of bone
tissue engineering is the generation of tissue-engineered grafts,
which includes cell seeding, culture, induction, and transplantation
(Fig. 26.10). Cultured cells can be seeded directly onto the scaf-
fold, induced into osteogenic cells, and then transplanted. Alterna-
tively,cellsculturedinflaskscanbeinducedintoosteogeniccellsand
detachedfromtheflaskatthetimeofsurgery.Thesearethenmixed
withthescaffoldfortransplantation.Forthegranular-typescaffolds,
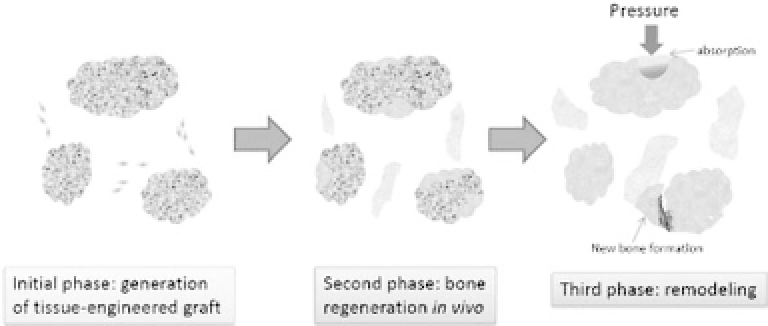
Figure 26.10.
The process of clinical bone tissue engineering can be
divided into at least three phases. The initial phase of bone tissue engi-
neering is generation of tissue-engineered grafts. Autologous BMSCs are
seeded on scaffolds before or after osteogenic induction. The scaffolds with
cells are then transplanted. The second phase is the process of bone regen-
eration. During this phase, scaffolds are degraded as new bone formation
occurs, which continues until the scaffolds are completely degraded. The
third phase is the process of bone remodeling after bone regeneration and
scaffoldabsorption.Thevolumeofregeneratedboneisregulatedbycoordi-
nated bone resorption and formation, which are affected by various local
and systemic factors such as pressure from surrounding soft tissues and
physiological loads from the dental implant.








Search WWH ::

Custom Search