Biomedical Engineering Reference
In-Depth Information
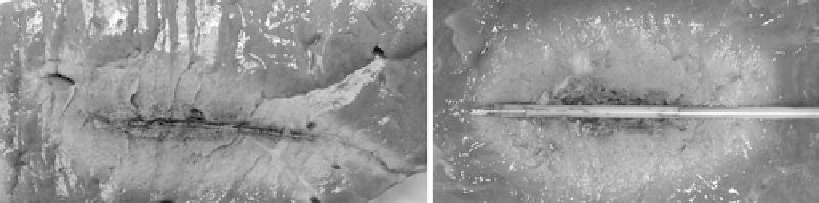
FIGURE 9.15
Microwave ablations created with uncooled (left) and water-cooled (right) applicators.
energy radiated from a single-point source. Ignoring any tem-
perature or perfusion effects, a constant energy inflow would
be expected to produce a constant spherical diffusion of heat—
that is, a constant increase in ablation zone volume (much
like the inflation of a balloon). However, since the radius of
the ablation zone is proportional to the cube-root of the vol-
ume, diametric ablation zone growth slows as the ablation vol-
ume increases (Figure 9.16). There are diminishing returns to
using a single radiation source for large-volume ablation for
extended time periods.
Second, the temperature profile across any thermal ablation
is not consistent, typically containing a peak near the applica-
tor and exponential decay toward the periphery of the abla-
tion zone. Most of the applied energy is also absorbed near the
applicator. The result is that once an initial ablation zone has
formed, additional energy primarily heats tissue that is already
necrotic, contributing only to maintain or increase the tem-
perature gradient across the ablation zone. This effect may be
more or less pronounced because of inherent changes in the
tissue properties of ablated tissue. Therefore, the concept of
spatially distributing the available power by using deployable
or multiple-applicator arrays has seen increased interest in
recent years.
9.5.3.2 antenna arrays for Microwave ablation
Studies have demonstrated that power can be more efficiently
distributed by using an array of antennas, even when compared
to a single antenna delivering the same total power (e.g., 90 W in
a single antenna versus 30 W in three antennas spaced 1-2 cm
apart in a triangular configuration; Laeseke 2010). In addition,
heating produced simultaneously by multiple sources in prox-
imity is known to produce ablation zones larger than might be
expected from a sum of each source. Several recent studies have
confirmed this
thermal synergy
when using arrays for RF and
microwave ablation, producing ablations up to 7 cm in diameter
(Brace 2009b, Oshima 2008, Laeseke 2006, Lee 2007, Yu 2006,
Simon 2006, Wright 2003).
Numerous studies of phased-controlled antenna arrays for
microwave tissue heating have been described in the hyper-
thermia literature (Jones 1989, Furse 1989, Lyons 1984, Turner
1984, Trembly 1985, Trembly 1986, Turner 1986). The objec-
tive of many of these studies was to produce a precise zone of
low-temperature hyperthermia (41-45°C) in a target area with-
out heating surrounding structures. Similar investigations for
high-temperature microwave ablation are ongoing. One poten-
tially detrimental effect of antenna interference can occur if the
relative phase is not known or controllable, as with multiple-
generator multiple-antenna systems. Under this condition, the
relative phase between antennas is unknown, and the result-
ing interference may be constructive or destructive, leading to
unpredictable results (Lubner 2010). It is currently unknown
how much clinical impact random phase has on the final abla-
tion zone. As an alternative, power may be switched between
antennas in the array to eliminate interference, producing more
predictable results (Brace 2007c). More study is needed to opti-
mize and control power produced by antenna arrays for micro-
wave ablation.
6
5
4
3
eory
Ex vivo
In vivo
9.6 Microwave ablation Conclusions
2
1
In conclusion, microwave ablation is playing an increasingly
important role in the treatment of many medical conditions.
In most cases, devices and equipment used clinically are in
their first or second generation. Recent developments includ-
ing cooled systems to increase power delivery, antenna arrays
to distribute power spatially, and optimization of technology
and technique based on specific tissue targets have already
0
0
5
10
15
20
25
30
Time (min)
FIGURE 9.16
Ablation zone diameters predicted using a constant
volumetric growth (theory), or simulations in
ex vivo
or
in vivo
liver.
Note the trend of decreasing diametric growth with time.