Biomedical Engineering Reference
In-Depth Information
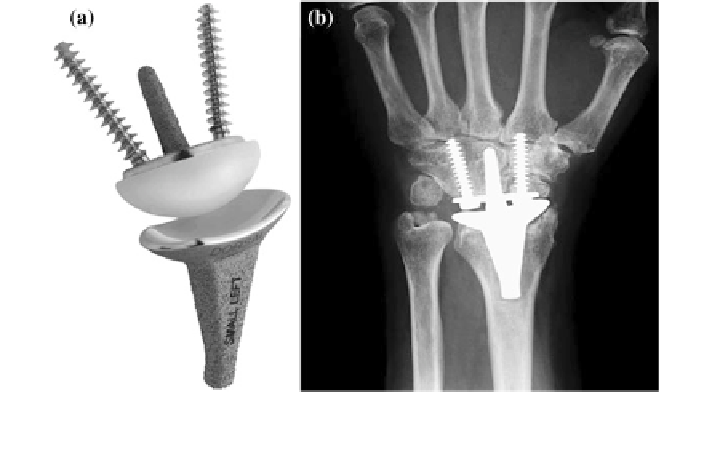
Fig. 3.5 ReMotion (Small Bone Innovations, Morrisville, PA) used in this arthroplasty as a
treatment for severe wrist affected by rheumatoid arthritis [
25
]
relief of pain while promising joint stability. Despite of its benefits, this procedure
will not be recommended for patients with both limbs affected, as it prohibits
motions of the limbs. It wills definitely causing difficulties to perform their daily
activities. To circumvent this problem, motion-preserving procedure has been
introduced.
Designed to preserve joint motions, total wrist replacement (Fig.
3.5
) or total
wrist arthroplasty (TWA) was established [
22
]. Similar to other joints, it requires
removal of some portions of the affected joint to place the implant. Despite of
promoting benefits, this technique resulting in high failure rate, primarily due to
metacarpal perforation and loosening of the implant [
22
]. Although numerous
attempts through designs of better implants and more efficient procedure were given
to improve this option, there are still many complications reported [
6
,
8
,
23
,
24
].
References
1. Viegas SF, Patterson RM, Hokanson JA, Davis J (1993) Wrist anatomy: incidence, distribution,
and correlation of anatomic variations, tears, and arthrosis. J Hand Surg 18(3):463-475
2. Dacho AK, Baumeister S, Germann G, Sauerbier M (2008) Comparison of proximal row
carpectomy and midcarpal arthrodesis for the treatment of scaphoid nonunion advanced
collapse (SNAC-wrist) and scapholunate advanced collapse (SLAC-wrist) in stage II. J Plast
Reconstr Aesthet Surg 61(10):1210-1218
3. Elhassan B, Shin AY (2009) Management of wrist arthritis secondary to advanced Kienbock
disease. Tech Orthop 24(1):27-31
4. Hogan CJ, McKay PL, Degnan GG (2004) Changes in radiocarpal loading characteristics
after proximal row carpectomy. J Hand Surg 29(6):1109-1113
Search WWH ::

Custom Search