Biomedical Engineering Reference
In-Depth Information
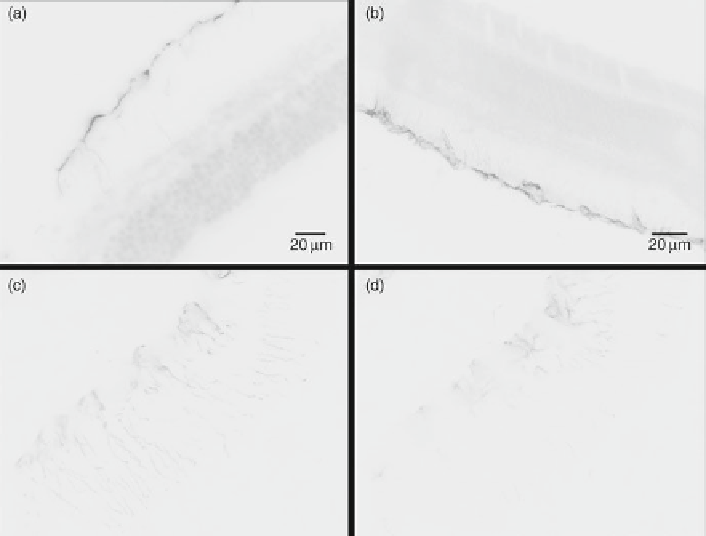
Fig. 7
Specifi c labeling of GFAP upregulation in the rat neural retina at a laser-induced lesion site
imaged using standard FITC ICC. (
a
,
b
) Wide-fi eld nonconfocal standard ICC using an anti-
GFAP-conjugated primary antibody and FITC fl uorophore-tagged secondary antibody. A nonspe-
cifi c nuclear DAPI stain was used to visualize the other retinal layers. (
c
,
d
) Confocal imaging of
two different lesions with a 1.6-mm optical slice and an acquisition time of 2 s, comparable with
the data shown in Fig.
2
. (
c
) Shows a slice near the center of a lesion while (
d
) shows a slice closer
to the boundary of a lesion. Note the particularly high background and diffuse labeling in (
d
).
Reproduced from Pathak et al. (
2009
)
(slices 4-6), followed by a progressive visible decrease in reactivity near the other
side of the lesion boundary (progressively from slice 7 to 9). Therefore, this labeling
method should be amenable to quantitatively measuring the extent and thickness of
glial scars and presumably other neuronal- and glial-specifi c markers in neural tissue
preparations at high spatial resolutions due to the cellular specifi city and low back-
ground of the procedure. Such an approach would conceivably allow better quantita-
tive measurements and statistics of both physiologically normal and, as illustrated
here, pathological cellular processes. This quantum dot-labeling procedure is consid-
erably superior to nonconfocal wide-fi eld epifl uorescence microscopy of retinal sec-
tions for specifi c labeling and imaging of GFAP upregulation in gliosis due to diffuse
labeling and higher nonspecifi c background in the latter (Fig.
7a, b
), as introduced
above. In our hands, the quantum dot-labeling procedure was subjectively less dif-
fuse, more intense, had a noticeably lower nonspecifi c background, and showed more
cellular detail than the best-optimized standard FITC ICC labeling we could achieve
(Fig.
7c, d
). This was especially true near the border of imaged lesions, where GFAP