Biomedical Engineering Reference
In-Depth Information
11.1 IntroduCtIon
The human pelvis, the lower part of the trunk, includes the bony pelvis, cavity, floor, and the
perineum. The pelvic skeleton is a complicated mechanical structure. It is formed by the sacrum
and a pair of iliac bones, which connect the spine with the lower extremities. The two iliac bones are
attached to the sacrum posteriorly with the sacroiliac joints (SIJs), articulated with the two femurs
with the hip joints, and connected to each other anteriorly with the symphysis pubica.
Surgical treatment of highly aggressive and malignant tumors originating from the pelvis is
always challenging due to the complex anatomy of the pelvis and the proximity of neurovascular
structures and viscera (Campanacci et al. 2012; Cheng et al. 2011). Partial resection of the pelvis
is still necessary in some patients (Grimer et al. 2013). Enneking and Dunham (1978) proposed a
classification scheme for describing the various subtypes of pelvic resection. A modified scheme
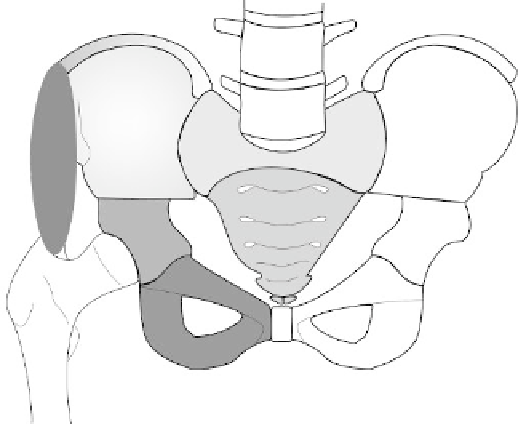
is shown in Figure 11.1. The resection locations were classified into several regions (Hosalkar
and Dormans 2007). Depending on the lesion location and extent, Enneking and Dunham (1978)
performed three types of procedures individually or in combination: (1) wide excision or radical
resection of the iliac wing; (2) periacetabular wide excision or radical resection; and (3) wide exci-
sion or radical resection of the pubis.
However, partial resection of the pelvis can cause trouble sitting, standing, and fitting a prosthe-
sis to the patient after amputation (Sneppen et al. 1978; Hoffmann et al. 2006). The continuity of
the pelvic ring must be restored to achieve structural stability and mechanical function following
hindquarter amputation. There are various options for reconstructing the pelvic ring after partial
amputation, such as arthrodesis, prosthesis, autograft, and allograft prosthetic composite recon-
structions (Campanacci et al. 2012). Each of these methods has its inherent advantages and limita-
tions (Hugate and Sim 2006).
The biomechanical properties of any implant must be evaluated to meet the stability and
mechanical requirements of reconstructive surgery. Some in vitro experiments have been under-
taken to study the biomechanical behavior of various surgeries (Yu et al. 2010; Cheng et al. 2011;
Mindea et al. 2012), but the measurable parameters in cadaveric experiments are very limited as the
experiments are very costly and samples are not easily acquired. Biomechanists and surgeons need
cheaper and more effective methods of studying relevant subjects.
I
IV
A
S
II
III
A
FIgure 11.1
(See color insert.)
Types of pelvic resection. The red oval indicates the gluteus medius mus-
cle; Type I = resection of the ilium; Type II = resection of the periacetabular region; Type III = resection of
the ischiopubic region; Type IV = en bloc excision of the sacral ala; A = aggressive resection; S = sacrum.
Search WWH ::

Custom Search