Biomedical Engineering Reference
In-Depth Information
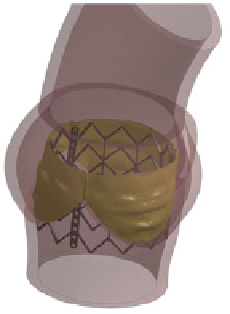
Fig. 6
Post-implantation configuration of model P2
Ta b l e 1
Average external radius and distal orifice area of the post-implanted stent configuration
in the three models (H, P1, P2)
Model H
Model P1
Model P2
Average external radius (mm)
13.1
12.6
12.6
Distal orifice area (cm
2
)
5.1
4.3
4.0
Ta b l e 2
Contact forces
computed on the LVOT and
on the AV in the three models
(H, P1, P2)
Contact forces (N)
LVOT
AV
Model H
12.6
9.7
Model P1
6.2
45.3
Model P2
6.6
50.8
0.5mm for the implanted Edwards Sapien
device and also in
accordance to in vivo CT measured distal orifice area [
26
] that reported average
values of 4.0
radius of 12.9
±
0.5 cm
2
. The distal orifice area of models P1 and P2 is also similar
to the values reported by Capelli and colleagues in their computational study [
13
].
The distortion of the post-implanted stent configurations was investigated, by
computing the normalized radius along the axial direction of the stent. The results
obtained in the three models are shown in Fig.
7
a. Model P2 showed the higher degree
of distortion (Fig.
7
b): in thismodel the stent configurationwas distally less expanded,
where the stent interacts with the native AV at the commissural level. In the light of
these results it can be claimed that the degree and location of calcifications on the
stenotic AV could affect the outcomes of TAV implantation, potentially interfering
with the expansion of the TAV stent.
The interaction between the stent and the anatomical structures was also analyzed:
the interaction forces were computed separately on the LVOT and on the AV in the
three models (Table
2
).
A different trend was observed between the healthy and the pathological models:
in the former, the interaction mainly affected the LVOT, while the forces acting
±