Biomedical Engineering Reference
In-Depth Information
echocardiography [
23
], suggesting that the strategy adopted in the present work
to model AV calcifications could represent a feasible approach when investigating
the macroscopic dynamic behaviour of stenotic AVs.
As concerns the mechanical loadings acting on AV models during the cardiac
cycle, pathological models experienced higher level of stresses particularly in the
belly region, where the average first principal stress reached 500kPa inmodels P1 and
P2 and exceeded by 11% the corresponding value computed in model H (450kPa).
Although somewhat trivial, this result could suggest interesting implications from
a pathogenetic point of view: it is well known that the origin and progression of
the degenerative aortic stenosis is strictly correlated to higher localized mechanical
stresses on the AV leaflets that could lesion the endothelium and start the fibrotic
process [
24
]; in the light of this result it can be speculated that the degenerative
process of AV stenosis could be self-enhanced and that the rate of progression of the
lesion could increase after the onset of the pathology.
3.2 TAV Simulations
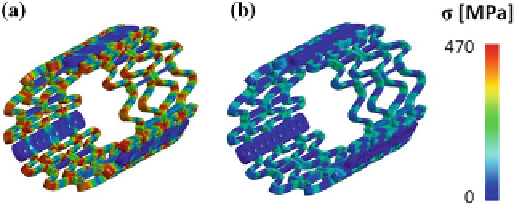
Concerning TAV simulations, in the stent crimping phase mechanical stresses were
higher at the joints of the beams where plastic hinges formed (Fig.
5
a). In those
regions, average Von Mises stress and plastic deformation reached 425MPa and
13.8%, respectively. After the recoil phase, the stent recovered part of the elastic de-
formation, but because of the non-uniform plasticization, a residual auto-equilibrated
stress field remained (Fig.
5
b). As a result of the elastic recoil, the external radius of
the stent increased from 4.7 to 4.9mm when the rigid planes were removed, which
corresponds to a percentage recoil of 4.3%.
In Fig.
6
the post-implantation configuration of model P2 is reported as an example
of the results obtained from the deployment simulations.
The stent configuration in the three models was characterized in terms of average
external radius and distal orifice area (Table
1
).
In the two pathological models a lower degree of stent expansion was achieved.
Results were in agreement with in vivo CT data [
25
] that reported an average external
Fig. 5
a
Von Mises stress in the stent in the end of the crimping phase and
b
of the recoil phase