Biomedical Engineering Reference
In-Depth Information
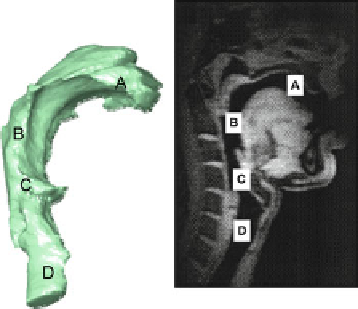
Fig. 12.8
Adult upper
respiratory tract from MRI
scan. Region A = oral cavity;
B = pharynx; C = larynx
opening into pharynx;
D = larynx (
From (
[
31
]
—
external view) and (
[
32
]
—
MRI image)—used with
permission
)
in the amount of inertial impaction that occurs in the upper airways from one patient
to another, which in turn controls the mass of aerosol able to penetrate further into
the respiratory tract and reach the airways of the lungs [
2
].
Given the importance of the upper respiratory tract geometry to the resulting
aerosol deposition profi le in the lungs [
30
], an obvious refi nement to the AIM-
pHRT concept would be to replace the compendial inlet with an anatomically cor-
rect throat model. One of the better examples is the model produced from MRI
studies facilitated in the early 2000s by the Oropharyngeal Consortium, comprising
three leading pharmaceutical companies, namely, AstraZeneca Research and
Development, Aventis Pharma, and GSK plc [
31
]. The consortium members sought
to understand the response of the human oropharynx to OIPs and the subsequent
effect of that response on the lung dose of inhaled medication. As a fi rst step to
achieving these aims, structural information of the oropharyngeal region was
required. The resulting model, an example of which is shown in sagittal view in
Fig.
12.8
, was developed with human volunteers during an appropriate inhalation
maneuver [
32
].
Given the diffi culty in agreeing upon a standard adult upper airway anatomy and
commercializing such a model, it is likely to be more convenient to make use of the
“Alberta” idealized adult anatomic throat (AIT) geometry that has been developed
and extensively validated by Finlay and colleagues in the early 2000s [
33
-
36
]
(Figs.
12.9
and
12.10
).
Even making use of this model, there is still the limitation that currently there
are no similar models yet commercially available to support in vitro studies to
determine the performance of OIPs intended for infants and small children, in
which the anatomy differs signifi cantly from that of an adult [
37
], including the
presence of obligate nasal breathing [
38
]. However, at the time of writing, this posi-
tion may be about to change [Copley M (2012) Copley Scientifi c Ltd, personal
communication], given the recent validation of an idealized child upper airway
inlet [
17
].
Search WWH ::

Custom Search