Biomedical Engineering Reference
In-Depth Information
60
Line of identity
40
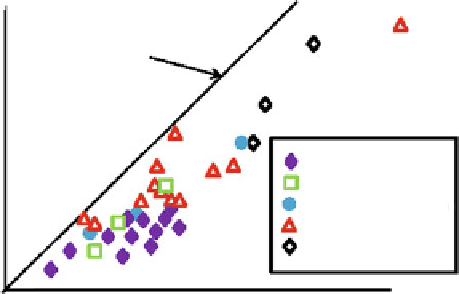
CFC pMDI
HFA pMDI
CFC pMDI + add-on
20
MDI
SMI
20
Fine particle fraction, % (<6.8
40
60
80
μ
m diameter)
Fig. 12.6
Correlation between mean whole lung deposition (gamma scintigraphy) and mean
FPF
<6.8 µm
by MSLI, for 33 inhalers (
From
[
2
]
—used with permission
)
It is conjectured that the incorporation of more realistic models of the upper
respiratory tract may offset some or all of the consistent bias observed in CI mea-
surements comparing whole lung deposition with CI-measured
FPF
<6.8μm
reported
by Newman and Chan [
2
] (Fig.
12.6
).
Their analysis collected data using the USP/Ph.Eur. induction port for 33 inhal-
ers representing all classes of OIP. Importantly, Newman and Chan observed that
when a glass bulb inlet to the MSLI was used, all the DPI data lay on the same
regression line, but the data point for the MDI group lay away from the line [
2
].
After replacing the glass bulb inlet to the impinger with a nonstandard inlet made
from an anatomical cast of the oropharynx, the data for all inhaler classes, including
the MDIs, lay on a single regression line. In consequence, they suggested that an
anatomical inlet to the MSLI would allow for more ready comparison between
inhalers of different classes. It would therefore seem reasonable to extend this con-
clusion to the other CI types, given that the differences observed appeared to be
related to the aerosol transport behavior upstream of the APSD measurement
apparatus.
In this context, as a further refi nement towards the realization of clinical reality,
an inlet having a fi xed internal geometry would not be able to refl ect changes in
particle deposition brought about by variations in oral cavity volume. Such effects
happen with real patients if they use devices with different mouthpiece dimensions
and are consequently opening their mouth wider or less wide [
15
]. Although ana-
tomically correct inlets having varying oral cavity volume are the obvious solution,
use of such inlets has practical complications associated with them (e.g., simulation
of the mucosa, drug recovery from the complex geometries of the interior surfaces).
The recent development of anatomically correct models developed from 3D MRI
scans of live patients should provide at low-cost aerosol transport conditions as
close to those in reality as is possible for such in vitro systems [
16
].
Search WWH ::

Custom Search