Information Technology Reference
In-Depth Information
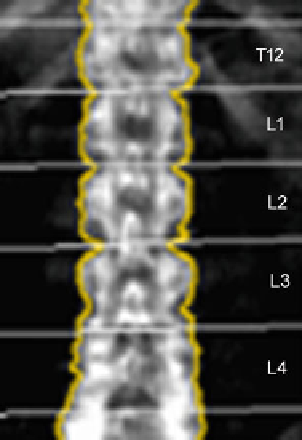
Fig. 6 Representative DXA
image from T12 to L4.
Measurements of areal BMD
(mg/cm
) are obtained for
each vertebra
measured BMD
subject
mean BMD
age
matched population
standard deviation BMD
age
matched population
Z-score
¼
The radiation dose for DXA measurements is relatively low and amount to
0.013
Sv at the spine [
29
]. BMD can be accurately determined by DXA which is
particularly important
μ
for
the longitudinal assessment of
treatment
response.
Reproducibility errors expressed as coef
cient of variation (CV) ranged between
1.0 and 1.5 % for the spine [
45
]. However, aortic sclerosis, degenerative disc
disease, and scoliosis represent signi
cant error sources for DXA-based BMD
measurements.
Quantitative computed tomography (QCT) at the spine avoids these error
sources. QCT-based BMD measurements at the spine are performed with clinical
whole-body multi-detector computed tomography (MDCT) scanners and are
determined as volumetric values in mg/cm
3
calcium hydroxyapatite [
46
]. Thus,
BMD values obtained by QCT are not size dependent in contrast to DXA-based
areal BMD. A further advantage of QCT is the separate measurement of cortical
and trabecular BMD (Fig.
7
). Since the trabecular compartment is the metabolically
more active one, treatment response can be assessed more accurately by using QCT
compared to DXA. QCT-based BMD is usually measured in the lumbar vertebrae
1
L3). Subjects with a trabecular BMD averaged from L1 to L3 between 80
and 120 mg/cm
3
are classi
-
3 (L1
-
ed as osteopenic and those below 80 mg/cm
3
as oste-
oporotic [
47
]. A calibration phantom in the table mat is required to be scanned with
the subject to convert the voxels
'
eld Unit into BMD
values in mg/cm
3
calcium hydroxyapatite. BMD measurements at the spine can be
performed as 2D single-slice QCT with a slice thickness of 8
attenuation values in Houns
10 mm. The scanning
-