Information Technology Reference
In-Depth Information
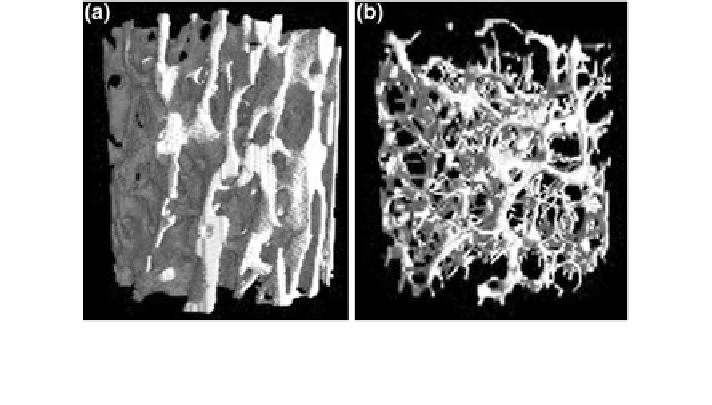
Fig. 1 Trabecular bone specimens of T10 from a normal (a) and an osteoporotic (b) subject. 3D
reconstructions of micro-CT scans with a spatial resolution of 26
μ
m
. Note the bone loss and
rare
cation in (b) compared to (a)
incident osteoporotic fractures amounted to 3.5 million, comprising 620,000 hip
fractures, 520,000 vertebral fractures, 560,000 forearm fractures, and 1,800,000
other fractures. The economic burden of prevalent and incident osteoporotic frac-
tures was estimated at
37 billion. Prevalent and incident osteoporotic fractures also
accounted for 1,180,000 quality-adjusted life years lost during 2010. Due to the
aging population, the prevalence of osteoporosis and consecutively the incidence of
osteoporotic fractures is expected to increase [
8
]. In the European Union, the costs
are expected to increase on average by 25 % in 2025 [
7
]. Similar projections have
been reported for the United States [
9
]. Therefore, osteoporosis is classified as a
public health problem.
The World Health Organisation (WHO) based the diagnosis of osteoporosis on
the measurement of BMD at the spine and hip using dual-energy X-ray absorpti-
ometry (DXA) [
10
]. Subjects with BMD values 2.5 standard deviations below the
mean of the reference population consisting of healthy young adult women are
classi
€
2.5), and subjects with BMD values ranging
from 2.5 to 1.0 standard deviations below the mean of the reference population are
classi
ed as osteoporotic (T-score <
−
1.0). However, T-scores and
BMD values of subjects with and without osteoporotic fractures overlap [
11
,
12
].
Schuit et al. [
11
] assessed in a prospective study baseline BMD and incidence of
non-vertebral fractures during follow-up in 7,806 men and women aged 55 years
and older. They reported that only 44 % of all non-vertebral fractures occurred in
women with a T-score below
ed as osteopenic (T-score between
2.5 and
−
−
2.5. In men, this percentage was even lower (21 %).
−
Similar
findings were reported for incident osteoporotic vertebral fractures [
12
].
Thus, the BMD thresholds for the pharmacological intervention to prevent fractures
are often inadequate. Subjects at high risk for osteoporotic fractures may not be
identi
ed and the necessary pharmacological treatment is not initiated. This is
particularly regrettable, since the current osteoporosis medications including