Information Technology Reference
In-Depth Information
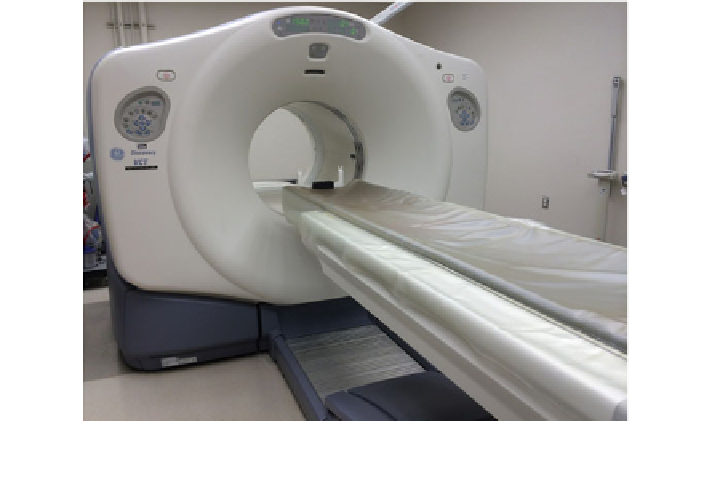
Fig. 17 PET/CT scanner unit. Patient is placed on movable table in alignment with the central
axis of the cylindrical scanner bore, with aligned sequential PET and CT scanners (note depth of
machine bore)
common usage in clinical practice is Technetium-99m (99m-Tc), which emits
140 keV gamma ray photons [
1
]. Radiotracers may either emit photons directly, or
emit particles which then decay and release photons. In either case, these photons
are then detected by varying geometry detector con
gurations, and are used to
produce cross sectional and volumetric images. Molecular imaging detectors
commonly used in clinical medical practice include gamma ray detectors used in
Positron Emission Tomography (PET) and Single Photon Emission Computed
Tomography (SPECT) scanners (Fig.
17
). The soft tissues of the body have a low
attenuation coef
cient for gamma rays, so the gamma photons pass through and
escape the body, and are detected by the scanner outside the patient. Emitted
photons from the normal regions of physiologic radiotracer distribution are used to
create a rough projection of the body anatomy. Foci of abnormal radiotracer
accumulation may be identi
ed superimposed over the expected normal distribu-
tion, indicating regions of pathologic processes. After imaging scan completion, the
complexed radiotracer molecules decay toward a stable state where they are no
longer radioactive, and in general as well, are physiologically excreted from the
body.
An advantage of molecular imaging is the ability to integrate information on the
spatial distribution of physiologic processes within the body tissues with quanti-
tative data from these processes. However, nuclear medicine imaging is lower in
spatial resolution as compared to CT and MRI, a disadvantage. Other disadvantages
of nuclear medicine imaging include the requirement for highly specialized
equipment or services to obtain radionucides for imaging, and ionizing radiation