Biomedical Engineering Reference
In-Depth Information
30,000
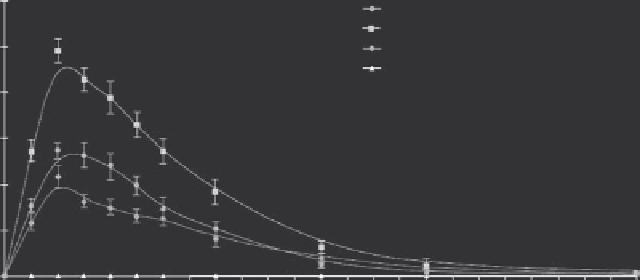
Liposomal doxorubicin
Total plasma doxorubicin
Unentrapped plasma doxorubicin
Total plasma doxorubicinol
n = 6
25,000
20,000
15,000
10,000
5,000
0
0
1
2 3
Time after start of infusion (hr)
4
5
6
FIGURE 16.9
Pharmacokinetics of liposomal and free doxorubicin in patients with liver tumors, treated with LTSL-Dox and thermal ablation at
the MTD dose of 50 mg/M
2
. (Reproduced from Poon, R. T., and Borys, N.,
Expert Opin Pharmacother
, 10, 2009. With permission.)
with a planned primary completion date of 2011 and study
completion date of 2013.
be dependent upon the type of drug that is loaded. The science
of drug loading into these nanoparticles is extensive, and each
type of drug formulation has to be carefully characterized and
optimized (Landon et al. 2011).
16.8.2.2 Chest Wall recurrences of Breast Cancer
Radiotherapy administered after surgical resection has impacted
local recurrences of breast cancer and has impacted survival
(Zagar et al. 2010). It is currently estimated that between 5 and
15% of breast cancer patients who receive radiotherapy will
experience a chest wall recurrence. The symptoms of such recur-
rences have substantial influence on the quality of life for these
patients. Symptoms can include pain, ulceration, bleeding, and
the distress of having a visible local failure (Zagar et al. 2010).
Hyperthermia has been used in combination with radiotherapy
for this disease and has been shown to be superior to radio-
therapy alone in randomized studies (Jones et al. 2005, Vernon
et al. 1996). This combination therapy has been approved by the
FDA for at least two decades. In spite of its relative success, local
failures are still common, which has led to the rationale to add
LTSL-Dox to hyperthermia as an alternate to thermoradiother-
apy. A phase I trial was completed at Duke last year using this
combination and results will be submitted for review soon.
16.9.1 additional applications for LtSL-Dox
The performance of LTSL-Dox provides strong rationale for
investigating its potential use in other diseases:
Liver metastases
. If the phase III trial for hepatocellular carci-
noma is positive, this would provide rationale for expanding its
applications for treatment of liver metastases.
Locally advanced breast cancer.
Locally advanced breast can-
cer is another potential target. This disease can be heated to the
proper temperature range, and there is experience in using non-
thermally sensitive doxorubicin containing liposomes in this
target population (Vujaskovic et al. 2010).
16.9.1.1 LtSL-Cisplatin and LtSL-Mitomycin C
As an example of the principles outlined before, we discuss, fol-
lowing, the rationale for clinical development of two LTSL for-
mulations that are targeted for treatment of bladder cancer. The
bladder is heatable, using the BSD 2000 family of RF-phased
array devices, so it is a good candidate site.
We have recently developed a cisplatin-containing LTSL, and
the first clinical application with this formulation will be for
muscle-invasive bladder cancer. Bladder cancer has the fourth
highest prevalence and fifth highest incidence of all solid tumors
(Altecruse et al. 2010, http://seer.cancer.gov/csr/1975_2007/,
based on November 2009 SEER data submission, posted to the
SEER Web site, 2010, Canadian Cancer Society/National Cancer
Institute of Canada 2005). When the cost of treating a single
patient from diagnosis to death is considered, it also ranks as the
single most expensive cancer to diagnose and treat (Botteman et
al. 2003, Riley and Lubitz 1989, Riley et al. 1995). Approximately
75% of new bladder cancers are nonmuscle invasive (NMIBC),
and such tumors are characterized by high local recurrence rates.
16.9 Future Directions
The choice of therapeutic payloads to consider adding to the
LTSL platform is dependent upon choosing diseases that might
benefit and then discerning whether such diseases are heatable
to the temperature range needed for drug release. Preferably,
one would want to use drugs for which there is thermal aug-
mentation of cell killing as well, although that is not an absolute
requirement. The success with LTSL-Dox that has been seen thus
far is below the temperature needed to see synergistic cell kill-
ing with hyperthermia (Hahn et al. 1975), for example. Choice
of drugs to load within liposomes is also dependent upon lipid
solubility. Drugs that are highly lipid soluble will be incorpo-
rated into the lipid bilayer as opposed to being in the aqueous
center, and the performance characteristics of drug release may