Biomedical Engineering Reference
In-Depth Information
TABLE 9.1
Electrical Tissue Conductivity at a Frequency of 500 kHz
(= RF ablation frequency)
0 s
30 s
Electrical current density
100%
Electrical Conductivity
σ (S/m)
Tissue Type
Reference
0.36
(Haemmerich 2003b)
Normal Liver
(rat,
in vivo)
Liver Tumor
0.45
(Haemmerich 2003b)
(rat
,
in vivo)
Myocardium
0.54
(Tsai 2002)
(porcine, in vivo)
Lung inflated
50
0.1
(Gabriel 1996b)
(porcine, ex vivo, 37°C)
Fat
0.02
(Pop 2003)
(porcine, ex vivo, 22°C)
Bone
0.03
(Gabriel 1996b)
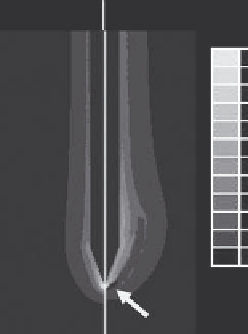
FIGURE 9.5
Electrical RF current density for cooled needle electrode
at beginning of ablation (left) and after 30 s (right). Due to tissue vapor-
ization around 100°C and associated drop in local electrical conductiv-
ity, current density drops after 30 s around the electrode tip (arrow),
since at this location temperatures above 100°C are obtained first.
Current density is shown as percentage of maximum. (Reproduced with
permission from Haemmerich, D., and Wood, B.J.,
Int J Hyperthermia
22, 2006b. Note also relationship between current density and SAR
[Equation 9.1].)
(porcine, ex vivo, 20°C)
Blood
0.7
(Gabriel 1996a)
(rabbit, ex vivo, 20°C)
Vaporized Tissue
~1e-15
Assumed same as air
discussion we will always assume this frequency range when
referring to electrical tissue conductivity. There is a large amount
of literature where electrical conductivity has been measured
experimentally in various tissues, typically from animals (Duck
1990, Foster 1989, Gabriel 1996a, Gabriel 1996b). It is important to
note that most of these studies were performed in extracted tissue,
since electrical conductivity changes rapidly after tissue removal
from the body (Haemmerich 2002, Tsai 2002). In Table 9.1 we list
the electrical conductivity of various tissues from measurements
in live animals whenever such data is available.
Since RF ablation is performed in soft tissue organs such as
liver, as well as in bone and lung, the differences in electrical con-
ductivity between these tissues are of relevance. In particular,
the low value reported for lung tissue (probably due to the pres-
ence of electrically insulating air inside lung alveoli) likely is one
of the reasons why RF ablation creates smaller ablation zones in
lung compared to other tissues (Brace 2009a). Also notable is that
multiple studies have reported differences between conductivity
of normal and cancer tissue (Esrick 1994, Lu 1992, Surowiec 1988,
Swarup 1991, Haemmerich 2003b), where tumor tissue has about
1.3 times higher electrical conductivity, likely due to loss of cell
membrane integrity associated with cell necrosis (i.e., cell death)
often present in tumors (Haemmerich 2003b).
Electrical tissue conductivity varies considerably with tem-
perature as already briefly discussed. An increased ion mobil-
ity with rising temperature results in a reversible increase
in electrical conductivity with a temperature coefficient of
approximately 1.5%/°C (Duck 1990). Once tissue temperatures
exceed approximately 50°C, irreversible changes are observed.
In one study electrical conductivity of kidney tissue was mea-
sured at temperatures up to 80°C, where permanent increase
in conductivity was observed above 50°C (Pop 2003). Similar
changes were observed in a recent study performed on surgi-
cally removed liver and tumor tissue from liver cancer patients,
where electrical conductivity was measured before and after tis-
sue ablation (Haemmerich 2009). The causes for these irrevers-
ible changes are not completely clear, but tissue dehydration and
changes in cell membrane properties may be two contributing
factors. At temperatures above 100°C (boiling temperature of
water), tissue begins to vaporize. Vapor has a very low electrical
conductivity (i.e., it is insulating, see Table 9.1), and therefore has
a large impact on RF current pathways. As shown in Figure 9.5,
current density drops at locations where vapor starts to form,
and heating at these locations is effectively eliminated.
9.3 Clinical applications of
radiofrequency ablation
9.3.1 Cancer treatment (aka
radiofrequency tumor ablation)
When thermal ablation using RF current was first clinically used
for cancer treatment, it was initially used for liver cancer (both
primary and metastatic) since for these patients often surgery
is not possible (~80% of patients) (Rhim 1999), and the other
two standard therapies—chemo- and radiation therapy—are
not effective due to biological reasons. Recent clinical studies on
patient survival suggest that with proper patient selection simi-
lar patient survival rates as with surgical tumor removal (the
current gold standard) are attainable (Gillams 2009, Livraghi
2008). In the last few years, tumor ablation has expanded to
other cancer types such as lung, kidney, bone, and adrenal gland
(Gillams 2008). Especially for lung cancer, tumor ablation has
received considerable attention, as there are more than 200,000
new cases of lung cancer reported annually in the United States