Biomedical Engineering Reference
In-Depth Information
recurrent breast cancer at the chest wall, the conditions can put
high constraints on the required equipment. Chest wall recur-
rences can be very localized (e.g., a treatment area of less than
100 cm
2
), or very huge with tumor growth extending over a
large part of or even over the whole chest wall (in case of cancer
“en curasse” even large parts of the back can be involved). In
the latter case it might be necessary to configure a treatment
strategy consisting of several sequential sessions in order to
heat the whole tumor volume. Frequently, the skin surface is
highly irregular due to previous surgery or tumors protruding
through the skin and with alternating tissue thicknesses vary-
ing between just skin and bone (ribs) to several centimeters of
heterogeneous fat-muscle tissue. Depending on the frequency
of the microwave fields, the rule of thumb is that the tumor
should not extend deeper than 2 or 4 cm for systems operating
at 915 or 434 MHz, respectively.
In addition, the strong spatial variations in tissue type, blood
perfusion, and anatomy require a high degree of control on the
spatial energy deposition. This can be achieved by using multi-
element antenna systems with power control per element.
Fortunately, modern clinical hyperthermia devices using
electromagnetic energy in the frequency range of 400−1000 MHz
do provide the flexibility required to adequately and com-
fortably heat this large variation in target volumes. Research
during the last three decades has delivered a number of
antenna designs that, when used with proper judgment, pro-
vide adequate heating characteristics for the circumstances. In
general the somewhat bulky and more ridged applicator types
like waveguides and current sheet antenna arrays operating
at 434 MHz are considered better suited to heat large nodular
types of tumors (exophytic and ulcerating) as well as recurrent
breast cancer with tumors growing to >2 cm depth, as they pro-
vide a higher energy deposition at depth. Conformal microwave
arrays are on the other hand the most suited applicator type
to heat large contoured areas of the torso, avoiding discomfort
from underlying ribs.
Academic and commercial devices for superficial hyper-
thermia that are successfully used for clinical application are
reported in Section 8.5.1.1.
(a)
(b)
(c)
8.5.1.1 academy-Based applicators
8.5.1.1.1 Lucite Cone Applicator [42,43]
The Lucite cone applicator (LCA) is a 434 MHz water-filled
horn applicator designed for external heating of superficial
malignancies (superficial hyperthermia). A conventional appli-
cator (CA) consists of a water-filled rectangular waveguide that
ends in a horn antenna. The LCA is a modification of the CA.
The waveguide is made of brass and operates at the TE
10
mode
at 434 MHz. The waveguide dimensions are 3 × 5 cm, and the
aperture size of the radiating antenna is 10 × 10 cm
2
. he two
diverging metal walls of the horn antenna, which are parallel
to the electric field, are replaced by Lucite walls. Additionally,
a PVC cone with a height of 5.5 cm is inserted in the applica-
tor at the center of the aperture. Compared to conventional
(d)
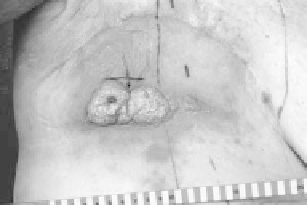
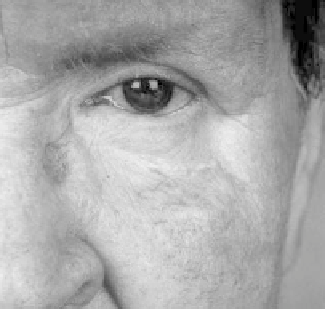
FIGURE 8.2
Two examples of patients referred for combined treat-
ment with radiotherapy (re-irradiation) and superficial hyperthermia to
demonstrate the large difference in location and thus requirements on
the equipment: (a) and (c) before treatment, (b) and (d) after treatment.
treatment has been reported include all parts of the body
(i.e., primary and recurrent tumors located at the skull, neck,
legs, arms, vulva, groin, back, and chest wall). Especially for