Biomedical Engineering Reference
In-Depth Information
From the beginning clinical studies were performed to evalu-
ate the clinical performance of the various deep heating systems.
In a direct clinical comparison, it was shown that the annular
array (AA) was superior to the concentric coil [30], and had an
equal heating efficiency to the Thermotron R.F. capacitive sys-
tem when used for patients with a fat thickness less than 1.5 cm
[31]. In a small study of eight patients, Shimm et al. [32] found
that with the air-coupled CDRH Helix (resonant helical coil)
system similar temperatures were measured as with the BSD-
1000 annular phased system. Despite all efforts, in approxi-
mately 90% of the clinical treatments with the BSD-1000 system,
local pain, general discomfort, and rise of normal tissue tem-
perature was power limiting with subsequently too low tumor
temperatures [32,33,34,35,36]. These findings quickly initiated
new applicator designs that all addressed in one or more ways
the reported limitations of the BS-D1000 Annular Phased Array
system.
The coaxial TEM applicator [37] was unique concerning its
open water bolus; due to the lack of water pressure on the skin
of the patient, a better treatment tolerance was realized. Due to
its simple electromagnetic design the coaxial applicator could
be used over a broad frequency range and needed only a single
high power generator. This of course was beneficial for quality
assurance and costs of equipment. Steering of the energy dis-
tribution was realized by moving the patient (i.e., the target
into the center of the applicator where the maximum energy
deposition was located). Salt water boli were used to reduce the
amplitude of the electromagnetic field at specified locations.
The ring applicator system as proposed by Franconi [38] and
van Rhoon et al. [39,40] was designed along the same prin-
ciple, but using lumped elements to couple the energy to the
applicator. With this ring applicator a circumferential E-field
distribution can be created from very low frequencies (27 MHz)
to frequencies above 70 MHz. Like the TEM applicator [37],
the ring applicator has the capability to adapt the axial extent
[39,40] of the energy distribution. An important advantage of
the ring applicator is its small size, which is comparable to that
of the Sigma-60 applicator. Additionally, elliptical applicators
have been studied to improve the SAR distribution [41]. The
introduction around 1990 of the BSD-2000 deep hyperther-
mia system with the Sigma-60 applicator as the successor of the
BSD-1000 system constituted a major improvement in equip-
ment. At the same time, the Amsterdam group introduced the
AMC four-waveguide system for deep hyperthermia [73].
%
100
TE10
434 MHz
50
20
Plane wave
10
3×3
5×5
5
8×8
20×20
10×10
2
1
0
10
20
30
40
50
60
70
80
mm
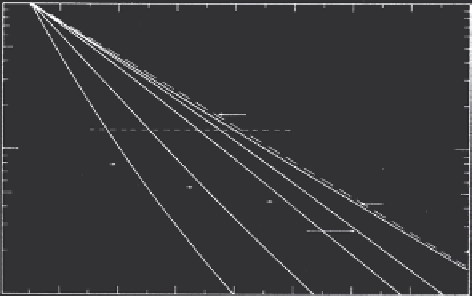
FIGURE 8.1
Absorbed power distribution as function of depth in a
muscle equivalent medium for 434 MHz and different applicator sizes
[28].
• Aperture size of the elements. Small elements will provide
high spatial resolution of power control and are capable of
conforming to body contour. As is well known and gen-
erally accepted [28,29], the penetration depth decreases
with smaller aperture size. As can be seen in Figure 8.1
the penetration depth for a single applicator with an aper-
ture of 10 × 10 or 5 × 5 cm
2
decreases from 22 to 14 mm for
the 25% SAR value and from 13 to 8 mm for the 50% SAR
value, respectively.
Eventually, these investigations brought us to the various
types of applicators for superficial hyperthermia that are cur-
rently used by several university groups and/or are sold by the
manufacturers of hyperthermia equipment.
For deep hyperthermia there was no equipment, other than
the capacitive and inductive devices from physical therapy,
available. From basic physics it was clear that the frequency of
the electromagnetic field should be low in order to obtain suffi-
cient penetration depth. Further, despite the increased penetra-
tion depth it was also clear that a single antenna element would
not provide sufficient energy deposition at the center of the
body. Consensus was rapidly reached that for “Western” patients
(i.e., with often a thick fat layer), only those electromagnetic
devices that generate a circumferential electrical field distribu-
tion around the patient, directed parallel to the body axis, are
capable of producing loco-regional deep heating. Several differ-
ent deep heating systems have been designed taking into consid-
eration the previously mentioned existing views and limitations
of equipment of the 1980s. One of the earliest radiative systems
available for deep heating was the BSD-1000 system. It consisted
of 16 waveguide antennas operating at a frequency of 70 MHz
and with synchronous settings (i.e., amplitude and phase of all
16 antenna elements were similar, leaving only control of the
total amount of energy delivered to the patient). In practice the
first users rapidly adapted the cable length between the antennas
such that they could dislocate the point of interference.
8.5 Currently available Systems
*
8.5.1 Devices for Superficial Hyperthermia
Patients referred for superficial hyperthermia represent many
different types of tumors (i.e., pathology, size, and location)
(Figure 8.2). Superficial tumor locations for which hyperthermia
*
This section on currently available systems is restricted to radiative elec-
tromagnetic applicator systems only!