Biomedical Engineering Reference
In-Depth Information
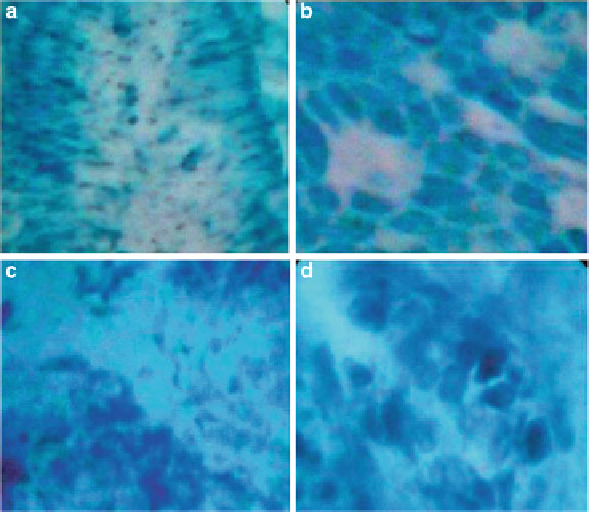
Fig. 8.17
Image produced by endocytoscopy in the human esophagus, in vivo, illustrating cellular
level features in normal tissue (
a
and
b
) and in squamous cell carcinoma (
c
and
d
).
a
,
c
and
b
,
d
correspond to 450 and 1,125 magnifications, respectively. Normal tissue demonstrates uniform
glandular structure, while abnormal tissue orientation of cells is random and irregular [
63
]
The use of endocytoscopy with chromoscopic dyes such as toluidine blue
primarily allows individual cell nuclei to be seen, with criteria such as nuclear
density, pleomorphism, and nuclear-to-cytoplasm area ratio used to differentiate
neoplastic from nonneoplastic mucosa. Figure
8.17
illustrates the type of image
produced by endocytoscopy in the human esophagus, in vivo, illustrating these
cellular level features in normal tissue and in squamous cell carcinoma. Endocy-
toscopy has been used to evaluate Barrett's esophagus, a recognized risk factor
for neoplastic transformation to adenocarcinoma, as well as cancers of the colon,
stomach, and lung. In terms of imaging parameters (FOV and resolution, working
distance), endocytoscopy is very similar to confocal endomicroscopy; however,
the images with the former technique tend to exhibit lower contrast, likely due
to the lack of optical sectioning. While the use of established dyes that are also
used in chromoendoscopy is appealing, the resulting range of tissue features that
can be observed (nuclear morphology) may be limited, with consequences for the
ability to identify neoplasia. Several pilot clinical studies have begun to evaluate
the diagnostic performance of endocytoscopy against histopathology [
63
]. A clear
advantage of endocytoscopy is its ability to provide cellular level information in
real time, enabling the endoscopist to inspect suspicious regions that are identified
Search WWH ::

Custom Search