Biomedical Engineering Reference
In-Depth Information
0.5
10
1
E
8
FCR
0.8
D
Torque
6
0.6
ECR
ECR
4
0.4
2
0.2
0
0
0
-2
-0.2
-4
-0.4
-6
FCR
-0.6
-8
0.5
10
-10
-0.8
0
0
1
1
2
2
3
3
4
4
5
5
6
6
7
7
8
8
9
9
10
0
20
40
60
80
100
120
140
t s
t s
(b)
(a)
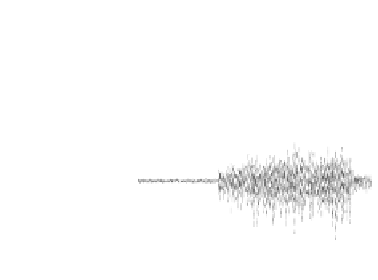
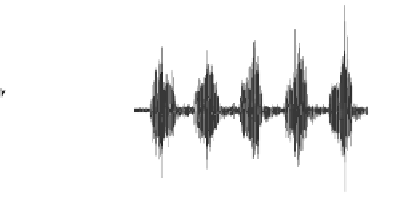
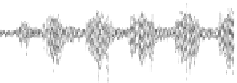
Figure 5.2
The representative EMG signals and torque signal obtained during isometric
maximum voluntary flexion at wrist joint of 0
◦
(a), and the representative EMG from the
FCR and ECR in a wrist tracking trial (b). For color reference, see page 215.
Besides the assistive torque, the interactive robotic system we developed also
could provide optional interactive resistive torque for challenge-based training.
The resistive torque could be applied in both flexion and extension directions,
that is,
T
r
=
a
·
T
MVC
,Flexion/Extension
(5.3)
where
T
r
,Flexion/Extension
was the resistive torque,
a
was the resistive coeffi-
cient (e.g., 10% or 20%, alternatively applied to the trials in a session), and
T
MVC
,Flexion/Extension
including two parts, the maximal
T
IMVF
(applied in the flex-
ion phase only) and
T
IMVE
(applied in the extension phase only). The net torque,
T
n
, provided by the robot during the training would be
T
n
=
T
r
,where
T
a
was
highly adapted to the muscle capability in a training session. It has been found
that applying resistance in tracking tasks may improve the muscle strength related
to the wrist movements (Hu
et al
. 2009).
T
a
−
5.2.2 Robot as an Evaluation System
Rehabilitation robot could share a large portion of the repeated labor work in a
long term physical training program, with the proper administration by a physical
therapist. Another advantage of using robot-assisted poststroke rehabilitation
training is that the robot could be a platform for quantitative monitoring on the
motor recovery process during rehabilitation training, due to the standardized
experimental setup and the high repeatability of training motions compared to
the modes manually offered. However, in many works on rehabilitation training,
only pre- and post-training evaluations were conducted to assess the training
effects, even in most of studies related to robot-assisted rehabilitation (Volpe
et al
.
2004). The commonly used clinical scores include the Fugl-Meyer Assessment
(FMA) (Fugl-Meyer
et al
. 1975) for assessing voluntary motor functions, the FIM
instrument (Keith
et al
. 1987) for evaluating independency in the daily life, the
Motor Status Score (MSS) test (Ferraro
et al
. 2002) for voluntary motor assessment