Agriculture Reference
In-Depth Information
100%
0%
Infected
Unwell
Consult
G.P.
Notified as
“Food-
poisoning”
Sample
taken
Pathogen
found
Reported to
surveillance
system
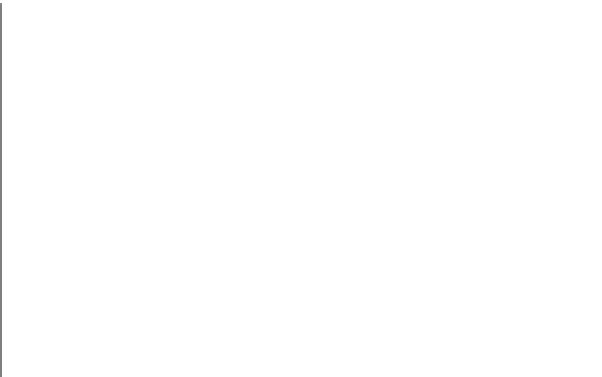
Figure 12.1
Surveillance for food-borne illness.
Laboratory reports of enteric infections
Routine reporting from medical laboratories gives a
useful picture of the importance of pathogens present
in the population. It does, of course, only record the
results from
samples
actually submitted to laboratories
and can therefore be distorted by any factors which
might influence sampling, for example, increased
media attention. Results can also be influenced by the
likely success of identifying a pathogen when present,
and this success may change as laboratory methodolo-
gies improve. For example, during the 1980s, better
techniques for the recovery of
Campylobacter
spp.
became routinely available, and this undoubtedly
contributed to the overall increase in numbers reported
during the 1980s and 1990s. However, since the early
1990s, methods have been standardised and should
not be the explanation for the continuing increase for
Campylobacter
spp., 200,000 reported EU cases in
2010.
Other extraneous events also play a part when iden-
tifying laboratory-confirmed cases. A change in policy
occurred when the Advisory Committee on the
Microbiological Safety of Food recommended in 1995
that
all
stool samples be screened for
Escherichia coli
O157. Previously, many laboratories were selective and
had perhaps restricted the examination for this organ-
ism to stools from children or from patients with
bloody diarrhoea.
The variation in laboratory methods and sample
submissions may partly explain the geographical differ-
ences seen throughout the United Kingdom.
infectious causes of food poisoning. It is estimated that
only between 1 and 10% of all food-borne illness is even
counted by the various surveillance systems, and this
varies from cause to cause (Fig. 12.1).
In any population, not all of those who become infected
become ill. Of those who are unwell, only a proportion
will seek medical help and can be counted as 'notifica-
tions. Those who do not require medical assistance are not
included in any surveillance system. If the clinician sus-
pects 'food poisoning, then that patient
may
be formally
notified, for which the GP will receive a notification fee.
The number of notifications may be supplemented, for
example, Health Officials and Environmental Health
Officers in the United Kingdom, including cases they
become aware of during their investigation. The doctor
may submit appropriate samples for laboratory investiga-
tion, and this forms the basis of laboratory surveillance.
The sample taken may affect the result; for example, vomi-
tus is more appropriate for a viral agent than is a stool
sample. Unless the sample is submitted within 24 hours of
onset of illness, a viral cause is likely to be missed. If a
pathogen is identified, then the result should be recorded
by the laboratory surveillance. When no pathogen is iden-
tified, it does not, of course, mean that none were present
but rather that the laboratory did not identify anything.
This will depend on the organisms under scrutiny. When
an outbreak occurs, it is likely that there will be greater
investigation of the source of infection than might be the
case when only a single patient is unwell. Causes of
outbreaks may be different from the causes of sporadic
infections, and it may not be possible to extrapolate.