Environmental Engineering Reference
In-Depth Information
(measured as TSP early on the cohort) made it dificult to distinguish PM and ozone-related
health effects [205]. A recent report from the Children's Health Study based on up to 5 years
of follow-up of children 9-16 years from 12 communities in southern California failed to ind a
clear association between PM aerosol and the onset of new asthma [206] (Table 23.12). An asso-
ciation with ozone was observed for children who participated in three or more outdoor sports
(Table 23.12). Other reports based on a follow-up of this cohort identiied important indoor and
familial factors as additional determinants of new-onset asthma [207,208], but no attribution of
risk was attempted between these latter exposures and ambient PM or other ambient pollutants.
Although the mechanisms by which PM aerosol could contribute to the onset of asthma in sus-
ceptible individuals are compelling, the data in Table 23.12 are not so compelling. As the MRC
study indicates, if PM aerosol and/or other ambient or indoor pollutants do contribute to the
risk of the asthma etiology, the effect is likely to be small and will be dificult to sort out from
other important exposures such as allergens and fungi. A further complication relates to the
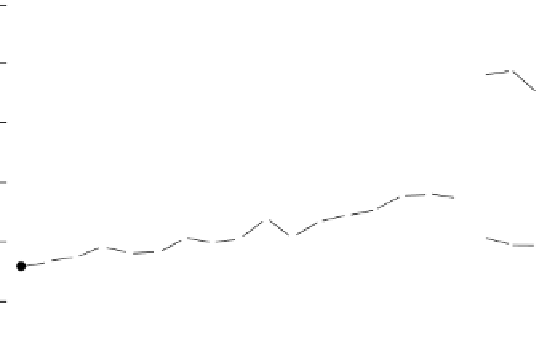
observation that the “epidemic” of asthma may have peaked, and asthma prevalence is declining
(Figure 23.21). If this is the case, and the mechanisms related to PM aerosol discussed earlier
are operative, then the focus of epidemiological studies will have to shift more intensely to the
identiication of the susceptible proiles with large populations.
A series of studies from Germany indicates that the connection between exposure to PM
aerosol and the occurrence of asthma and atopic allergy may involve different mechanisms or
a different time course in populations. With the fall of the East German Republic (1989) and
the uniication of Germany (1990), there was a sharp decline in levels of SO
2
(precursor of
secondary sulfate aerosol) [209]. Early studies indicated that the prevalence of atopic diseases
and asthma was
less
frequent in the old East German Republic and that symptoms of bronchitis
were more frequent [210]. Surveys carried out several years after the reuniication observed
that prevalences of atopic allergy and positive prick skin tests were now similar in former East
(Dresden) and West German (Munich) cities, but that the prevalence of asthma and reactive
Estimated annual prevalence
a
of asthma-United
States, national health interview survey, 1980-1999
120
Lifetime asthma
100
80
Asthma prevalence during the preceding 12 months
60
40
Episode of asthma or
asthma attack during
the preceding 12 months
20
0
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
Year
FIGURE 23.21
Annual self-reported prevalence of current asthma based on the National Health Interview
Survey. Note: Format of questions changed after 1996. Data demonstrate plateau in reported prevalence of
asthma in the preceding 12 months (current asthma) and report of asthma at any time during life. (From
Centers for Disease Control and Prevention,
MMWR
, 51, 1, 2002.)
a
Per 1000 population; age-adjusted to the
2000 U.S. population.
























Search WWH ::

Custom Search