Environmental Engineering Reference
In-Depth Information
Deposited particle
Endocytosis by
type I alveolar
epithelial cells
Blood
Phagocytosis by alveolar
macrophages
Passage through
pulmonary capillary
endothelium
Passage through
alveolar epithelium
Movement within
alveolar lumen
Phagocytosis by
interstitial
macrophages
Interstitium
Bronchiolar/bronchial
lumen
Lymphatic channels
Mucociliary blanket
Lymph nodes
GI tract
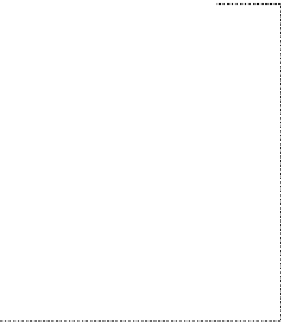
FIGURE 23.12
Known and suspected pathways for clearance of insoluble particles. This diagram does not
include all of the pathways for the clearance of bioaerosol particles such as fungal spores and viable bacte-
ria which may involve primary phagocytosis by polymorphonuclear leukocytes as well as macrophages and
other immunologically mediated effector mechanisms. Mucociliary blanket (transport) refers to the combined
effects of ciliary action of epithelial cells to the level of terminal bronchioles and mucus secretion by mucus
glands (only found in airways with cartilage [seven generations] and goblet cells [found to the level of respi-
ratory bronchioles]). (From Schlesinger, R.B., Deposition and clearance of inhaled particles, in McClellan,
R.O. and Henderson, R.F., Eds.,
Concepts in Inhalation Toxicology
, Taylor & Francis, Washington, DC,
pp. 191-224, 1995; Wanner, A. et al.,
Am. J. Respir. Crit. Care Med
., 154(6 Part 1), 1868, 1996.)
23.3.2 c
learance
*
Clearances of nonbiological and biological aerosol particles have many common elements, and
these are discussed in this section. These general pathways are depicted in Figure 23.12. The one
major difference between the clearance of insoluble nonbiological particles and particles that are
intact bacterial or fungal spores relates to the latter's activation of the complex immunological
pathways responsible for killing these agents. These latter processes are summarized very briely in
Table 23.4 and are not discussed further.
Particles that enter the nasal cavity are cleared largely by muciliary clearance (Figure 23.11
and Ref. [29]), sneezing, nose blowing, or dissolution for soluble particles. In the tracheobronchial
tree, poorly soluble particles are cleared by mucociliary transport (the net movement of which is
toward the oropharynx) and are swallowed or removed by coughing. More soluble particles may be
absorbed through the mucosa and enter the bloodstream.
Insoluble particles that reach the alveolar region of the lung are ingested by alveolar macro-
phages. Increasing particle burden results in increased numbers of cells, the maximum accumu-
lation of which appears to be more a function of particle number than of particle mass. These
particle-illed cells are cleared by the mucociliary apparatus, by migration into the connective
tissue that separates the alveoli (air sacs) and surrounding airways, and into the bloodstream via
lymphatic channels. Some of these latter particles may then migrate to lymph nodes that are located
along the tracheobronchial tree and then enter the bloodstream. Uningested, ultraine particles may
enter the bloodstream directly across the alveolar and capillary epithelium, and this clearance into
the blood can be very rapid. Within 1 min after human inhalation of
99m
Technetium-labeled car-
bon particles (<100 nm), labeled particles can be detected in the blood, with peak concentrations
*
This section is a synthesis of extensive discussions presented in Refs. [25,28].














































Search WWH ::

Custom Search