Environmental Engineering Reference
In-Depth Information
1.0
0.8
0.6
0.4
0.2
0.0
0
20
40
60
d
(nm)
80
100
120
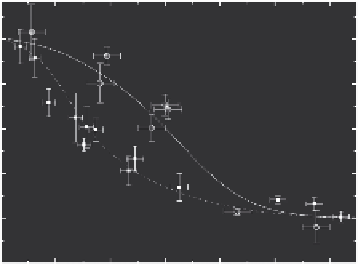
FIGURE 11.9
Mouse respiratory eficiency (ε) versus mean particle diameter; circles, the data for ibuprofen;
squares, the data from the indomethacin nanoparticle inhalation experiments. Bars, indicate standard error;
lines are given as eye guides. There is some discrepancy between the deposition eficiencies measured for
indomethacin and ibuprofen particles. One of the possible reasons for this discrepancy may arise from differ-
ent hygroscopic properties of indomethacin and ibuprofen nanoparticles.
fur deposition, two chambers were put in parallel, the same way as it was done in the inhalation
experiments. One chamber was empty and the other one was occupied by four mice. The ratio of the
particle concentration at the outlet of the occupied chamber (
n
out
) to that of the empty one
n
ou
( 0
was
measured to be (
n
= ± ). Thus, the total aerosol depletion in the occupied chamber
was about 15%. When evaluating the lung-deposited dose the average between inlet and outlet con-
centrations was used.
/
n
( )
0
0
.
91
0 0
.
2
out
out
11.1.2.3 Analgesic Effect of Ibuprofen Nanoaerosol
It is convenient to use the relative analgesic index (RAI), that is, the ratio between the mean num-
ber of writhes for the aerosolized group (or oral group) and that for the untreated group. During 1
day, one to three WB exposure runs were provided for aerosolized or oral groups and one run for
the animals from group 1 (eight animals per one run). Thus, during 1 day for all the runs of group
2 or 3, one and the same run of group 1 was considered as a match. Figure 11.10 shows the RAI
for the aerosolized animals as well as RAI for the orally treated animals versus the lung-deposited
dose. The RAI data for both the aerosolized and oral groups were analyzed for the dose-response
relationship. The itted curves are shown as the solid lines. Both aerosol and oral treatments give
no analgesic effect (RAI is about unity) at small lung-deposited or orally deposited doses (less than
10
−6
and 1 mg per kg bw for the aerosol and oral treatments, respectively). The regression analysis
applied to the RAI results showed that there was a statistically signiicant dose response (
R
2
= 0.91
and 0.96 for aerosolized and oral groups, respectively). Note that the lung-deposited dose was varied
by changing the heating temperature in the generator of nanoparticles; an increase in temperature
results in an increase of both the mean particle diameter and number concentration. Therefore, the
RAI points for different dose magnitudes correspond to different mean particle diameters. One can
also see from Figure 11.10 that the aerosol treatment is more effective (gives the same RAI for a less
dose) than the oral administration. The body-delivered doses for aerosol and oral treatments differ
by 3 and 5 orders of magnitude at the lung-deposited dose 10
−1
and 10
−4
mg per kg bw, respectively.
One of the reasons for this difference is probably the high level of metabolism of ibuprofen being
administered orally (Mutschler and Derendorf, 1995).
11.1.2.4 Anti-Inlammatory Effect of Indomethacin Nanoaerosol
Table 11.1 gives an example of the edema index for the groups 1 through 3 in the indometacin
nanoaerosol inhalation. The particle number concentration and mean diameter were 7 × 10
5
cm
−3
Search WWH ::

Custom Search