Environmental Engineering Reference
In-Depth Information
(A)
(B)
(C)
(D)
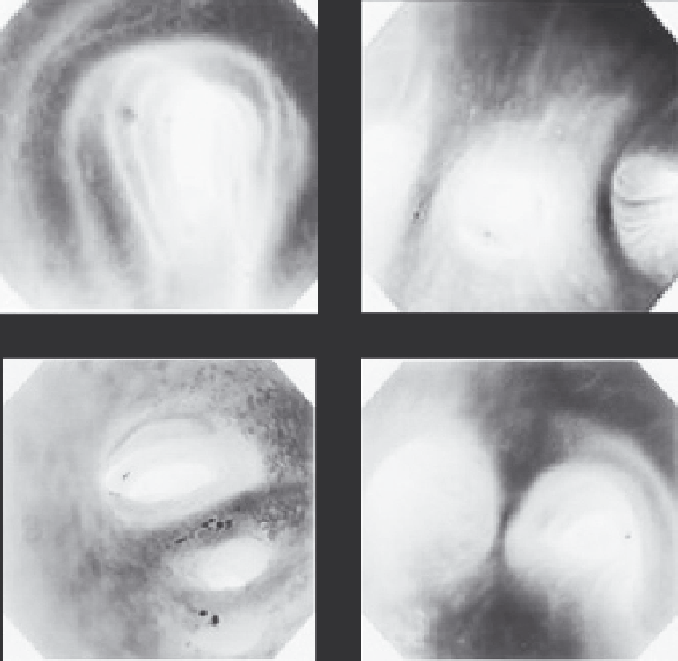
FIGURE 5.7
Airways and surface features photographed with videobronchoscopy. (A) The trachea and the
main bronchi with the cartilaginous rings clearly visible. (B) A quadruple bifurcation, indicative of the com-
plex branching pattern of the lung. (C) Blunt carinal ridges. (D) Sharp carinal ridges. (Reprinted with permis-
sion from Virtual Hospital, University of Iowa, Iowa city, IA, 1992-2003, www.vh.org.)
becomes so great that overcoming the relatively high pressure drop and resistance in the nasal passages
is no longer an eficient means of respiration. In healthy adults, the switching point between nasal and
oronasal breathing is thought to be approximately 35 L/min.
113,114
In children, however, this switch-
ing point is more variable.
115
Gender does not seem to play a role in switching point determination.
113
5.4.4.1.1 Effect of Oral or Nasal Breathing on Particle Delivery to Lungs
The route of breathing inluences the quantity of inhaled contaminants or therapeutics delivered to
human lungs. Particle penetration to the human lung is lower during nasal breathing (versus oral
breathing)
116
due to higher deposition eficiency in the nasal region, and there is thus more effective il-
tering of inhaled particles.
117,118
The higher deposition eficiency of nasal breathing is due to increased
particulate matter removal by nasal hairs, impaction on pathway walls, and diffusion. Thus, it is less
eficient to administer therapeutic aerosols to the human lung via the nose as opposed to the mouth.
5.4.4.1.2 Effect of Oral or Nasal Breathing on Total Particle
Deposition within the Respiratory Tract
Due to eficient particle removal by the nose,
119-121
total respiratory tract deposition is higher for
nasal breathing than for oral breathing in nonsmokers.
50,122
As stated, the higher deposition efi-
ciency in the nose versus the mouth is due to increased particle removal by nasal hairs, and inertial
Search WWH ::

Custom Search