Biomedical Engineering Reference
In-Depth Information
7
.
2
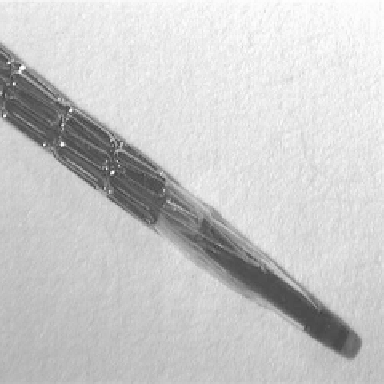
A typical metal stent mounted on the catheter tip. The image
shows the device prior to the balloon expansion.
vasculature the complete expansion of self-expanding stents is also aug-
mented by balloon infl ation. The stent is mounted by the manufacturer on
to a catheter tip (Fig. 7.2) and is positioned across the lesion. The appropri-
ate placement and positioning of the stent is guided by the use of intravas-
cular ultrasound (IVUS) (Mintz
et al.
, 1996) or fl uoroscopy, an imaging
technique which incorporates the injection of dye-contrast media into the
vessel and a fl uoroscope to provide an X-ray of the vascular architecture
and the stent (Putman, 1988). Infl ation of the balloon expands the stent
(and its positioning at the site of the atherosclerotic plaque), resulting in
an increase in the luminal diameter of the vessel, the sealing of intimal fl aps,
the limiting of vessel recoil and the reduction of vascular remodeling, pro-
viding a wider smoother lumen than balloon angioplasty alone (Fig. 7.3).
Vascular injury and bleeding complicate stenting but their occurrence has
been greatly reduced throughout the years due to the adoption of intensive
anticoagulation regimes (Langenhove
et al.
, 1996) including prolonged
heparinisation and the routine use of aspirin, clopidogrel, warfarin and
dextran. Stent-induced thrombus formation (blood clot formation in the
stent) has been classifi ed into (i) acute stent thrombosis, which typically
occurs within hours of the stenting procedure, and is typically due to incom-
plete stent expansion and/or vessel dissection, and (ii) sub-acute late stent
thrombosis which can occur up to 30 days after the stenting procedure.
Acute stent thrombosis has been dramatically reduced by the implementa-
tion of high pressure balloon expansion of stents decreasing the rate of
complications (Gandi & Dawkins, 1999).
Search WWH ::

Custom Search