Biomedical Engineering Reference
In-Depth Information
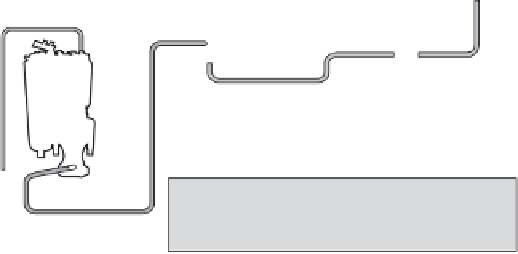
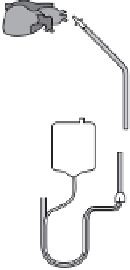
6.1
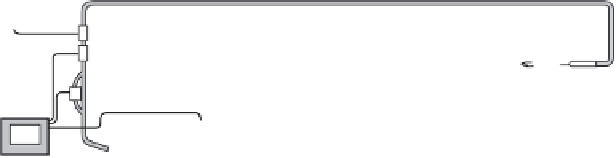
A schematic design of an extracorporeal circuit.
6.3 Basic principles of cardiopulmonary bypass
During CPB for clinical cardiac surgery, blood is typically drained by gravity
into the venous reservoir of the heart-lung machine via cannulae placed in
the superior and inferior vena cava or a single cannula placed in the right
atrium. Blood from this reservoir is pumped through a membrane oxygen-
ator into the systemic arterial system, usually through a cannula placed in
the distal ascending aorta. This basic extracorporeal perfusion system can
be adapted to provide partial or total circulatory and respiratory support
or partial support for the left or right heart or for the lungs separately (Fig.
6.1). Hypothermia reduces oxygen consumption by a factor of 0.5 for every
10 °C decrease in temperature. Dilution reduces perfusate viscosity, which
is not a problem during clinical CPB, but also reduces oxygen-carrying
capacity; mixed venous oxygen saturations below 60% usually prompt
either transfusion or increased pump fl ow. Porcine heparin (300-400 units/
kg IV) is given before arterial or venous cannulae are inserted. CPB is not
started until anticoagulation is confi rmed. Antegrade blood or crystalloid
cardioplegia is administered directly into the aortic root at 60 to 100 mmHg
pressure proximal to the aortic cross-clamp by a dedicated cardioplegia
roller pump. Prior to stopping CPB the patient is rewarmed to 34-36 °C, the
heart is defi brillated and the lungs are re-expanded (40 cm H
2
O pressure)
and ventilated.
5



























Search WWH ::

Custom Search