Biomedical Engineering Reference
In-Depth Information
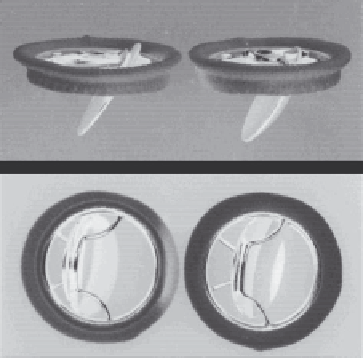
(a)
(b)
4.5
Björk-Shiley mitral valve prosthesis, with the tilting pyrolyte discs
in open position. Left, standard disc prosthesis; right, convexo-
concave disc prosthesis. Note the greater upward displacement of the
disc in the convexo-concave valve, compared to the standard valve
(a). The greater disc motion produces a larger valve area behind the
disc in the convexo-concave vs. standard valve (b).
However, despite the valve's apparently favorable hemodynamics, thrombi
tended to form on the outfl ow side of the valve. In 1975 a radiopaque ring
was added to the disc for fl uoroscopic detection of disc motion abnormali-
ties and clot deposition. In 1976 the disc was modifi ed from fl at to a con-
vexo-concave shape, and its pivot point was shifted 2 mm downstream. The
forward disc displacement enlarged the minor orifi ce by 12% at the expense
of the major orifi ce. These modifi cations improved the fl ow and decreased
the turbulence around the minor orifi ce (Fig. 4.5). Clinical reports indicated
improved hemodynamics and a decrease in thromboembolic events from
4.2 to 2.1% of patients per year.
Increasingly frequent reports of strut breakage (Fig. 4.6) and lethal disc
escape from the Björk-Shiley valves prompted an international study which
identifi ed several contributing factors including weld failure, large valve
sizes, and younger patients.
42,43
To address these problems, the entire valve
was machined from a solid piece of metal, and the housing was reconfi gured
to include only one outlet strut and to increase the disc opening angle to
70°. The modifi ed prosthesis, known as the Monostrut Björk-Shiley valve,
was released in 1983 for clinical use in Europe and Canada. The modifi ed
valve had a larger valve orifi ce area and reduced pressure gradients vs. its
predecessor,
44
and was found to be durable and associated with a low rate
of valve-related complications.
45
Search WWH ::

Custom Search