Biomedical Engineering Reference
In-Depth Information
Electrodes
Early transvenous leads had a relatively large electrode diameter (e.g., 4mm).
Irnich showed that the theoretical optimum (spherical) electrode radius for
stimulation was approximately 0.7±1mm, corresponding to the thickness of the
fibrous capsule layer that frequently forms around it (Irnich, 1973). Under a
given voltage, the highest electrical field should be in the tissue surrounding an
electrode of optimum size. However, determining the optimum electrode size is
a complicated matter. On one hand, a smaller size electrode has higher pacing
impedance, resulting in lower current drain and longer pacemaker longevity. On
the other hand, a smaller electrode has higher electrode polarization, which
affects its cardiac sensing functions and pacing efficiency.
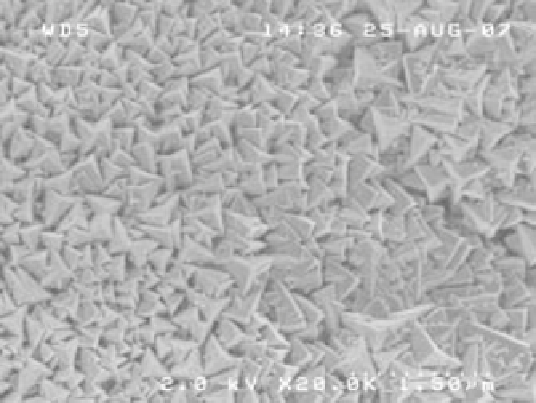
In the late 1970s, small electrodes with porous surface were introduced (Fig.
4.9). These structures produced high pacing impedance because of their small
size (radius), but their increased surface area from the porosity resulted in much
lower polarization, providing better sensing than polished electrodes. This
development solved the problem caused by the two constraints mentioned
above. The pores might also facilitate tissue ingrowth, which aided fixation to
the cardiac wall tissue. Porous surface coatings used today include platinum
black, titanium nitride, iridium oxide and activated carbon.
A problem for early lead electrodes was that the pacing threshold increased
over time. A pacing threshold is the minimum voltage electrodes need to apply
to tissues for them to respond. An increased threshold can cause failure of
pacing and/or increase in energy consumption that reduces the longevity of the
device. An increased threshold was found to be associated with inflammatory
4.9 Scanning electron microscope (20 000) of a titanium-nitride coated
electrode (courtesy of Medtronic, Inc.).