Biology Reference
In-Depth Information
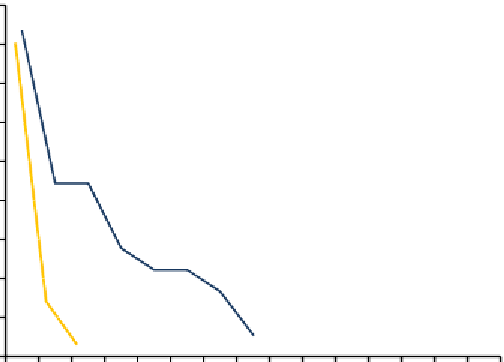
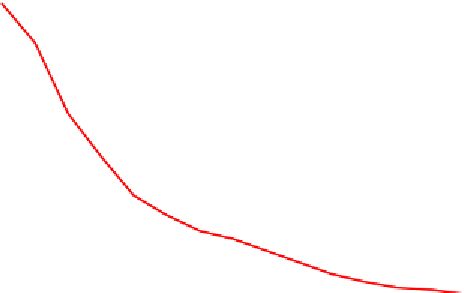
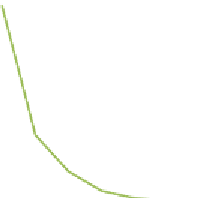
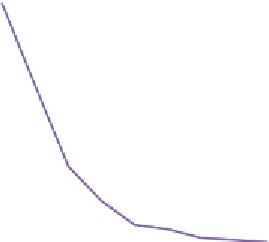
Figure 2.5
The proportions of patients experiencing successive
P. vivax
relapses taken
from eight different clinical series, described in detail in
White (2011)
. These were US
soldiers with vivax malaria acquired in the South Pacific (2 series), German soldiers who
acquired vivax malaria in Greece, US soldiers with vivax malaria acquired in the Mediter-
ranean area (two series) and Italy, patients receiving malaria therapy with a local 'strain' in
Moscow, British patients receiving malaria therapy with the Madagascar strain, patients
receiving malaria therapy with the McCoy strain in the United States, volunteers infected
with the Chesson strain in the United States and more recently children followed pro-
spectively in an evaluation of an ineffective malaria vaccine (SPf66) in north-western
Thailand. Inset shows proportions on a log scale and numbers of patients studied. For
colour version of this igure, the reader is referred to the online version of this topic.
the fraction of patients experiencing one or more relapses, then the frac-
tion experiencing
n
or more relapses is approximately
x
n
(
White, 2011
)
(
Fig. 2.5
). Thus, for areas with 50% relapse rates, approximately 12.5% of
patients have to have three or more relapses per incident symptomatic
infection. It follows that once symptomatic relapse rates exceed 50%, relapse
becomes the predominant cause of vivax malaria illness.
5. GEOGRAPHIC DISTRIBUTION OF RELAPSE
PHENOTYPES
Overall, there was good evidence for the presence of the long-latency
'Madagascar' relapse phenotypes in Europe, Southern Russia, North Africa,