Biology Reference
In-Depth Information
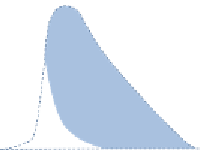
Figure 2.1
Long-latency
P. vivax
in the Netherlands a century ago. The mean monthly
number of malaria cases in the village of Wormerveer, The Netherlands, recorded by
Kortweg from 1902 to 1923 (black line) (
White, 2011
;
Korteweg, 1902
;
Swellengrebel
et al., 1936
;
Swellengrebel and De Buck, 1938
;
Winckel, 1955
). Swellengrebel et al.
showed anopheline vectors responsible for malaria transmission usually occurred
between the first week of August and the end of October. From this, it can be deduced
that the initial wave of malaria cases derived from inoculations the previous year (pink
curve) and, by subtraction, that this was followed by relapses and primary cases with
a short incubation period in the late summer and autumn (blue curve). For interpreta-
tion of the references to colour in this figure legend, the reader is referred to the online
version of this topic.
(
Swellengrebel and De Buck, 1938
). The pattern observed by James in
England, Swellengrebel in The Netherlands, and Ciuca in Romania with
the extensively studied Madagascar strain of
P. vivax
(
Fig. 2.2
) was very
similar to the relapse patterns of the St. Elizabeth and McCoy strains, of
indigenous origin, used for malaria therapy in the United States (
Tiburskaja
et al., 1968
;
Nikolaiev, 1949
;
Shute et al., 1978
;
Boyd, 1940a, 1947
;
Sinton,
1931
;
Boyd and Stratman-Thomas, 1933
;
Cooper et al., 1947, 1949
). These
strains were all chosen because of their suitability for malaria therapy, so they
probably represented the upper end of the spectrum of abilities to produce
early infection and relapse. Provided the initial illness was treated or atten-
uated by quinine, then relapse usually occurred approximately 9 months
later. These single-isolate (presumably single or highly related genotype)
infections eventually resulted in solid immunity such that after several epi-
sodes of protracted fever, reinfection with the same isolate was not pos-
sible (
Boyd, 1947
;
Boyd et al., 1936
). This acquired immunity suppressed
later genetically homologous relapses. The malaria therapy patients often
had no previous malaria, so any malaria recurrence must have arisen from