Biomedical Engineering Reference
In-Depth Information
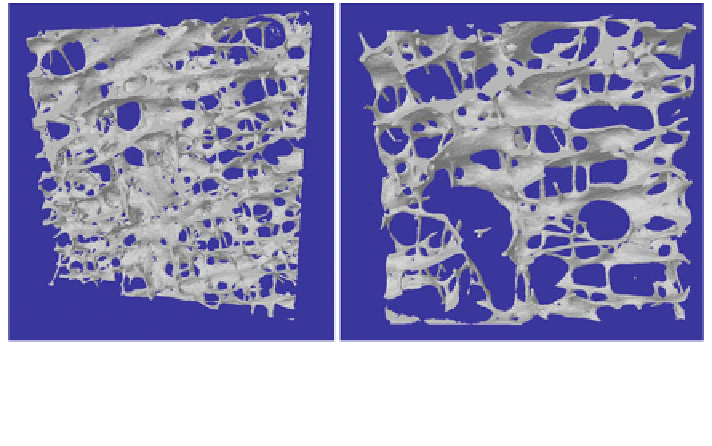
Fig. 8 3D rendering from micro-CT images of trabecular bone samples from human vertebral
bodies of two individuals, which have similar bone volume fraction but differ markedly in
architecture. (both samples were obtained from individuals over the age of 60, where the BV/TV
was 9.3 and 8.6%, respectively)
[
1
,
29
,
98
,
110
,
113
], particularly at sites with large load-bearing. During the 4th
to 6th decades and particularly before the menopause in women, the prevalence
of low-impact or fragility fractures is low compared to older age groups.
However, the incidence of fractures at sites such as the distal radius, the ribs and
ankles rises significantly after the age of 35 [
108
].
7 Trabecular Bone Structure in Older Age
Large and clinically relevant changes in trabecular bone structure occur from the
6th decade of life onward (Fig.
8
; Table
1
). The Rotterdam study [
96
] shows that
incidence of non-vertebral fractures in osteopenic and osteoporotic males and
females (diagnosed based on BMD t-scores) more than doubles after the 7th
decade. Fracture risk is site dependent and males and females have different dis-
tributions of prevalence in sites of fracture, for example the incidence rate per
1,000 person years for hip fractures in males is 3.0, whereas the incidence rate per
1,000 person years for females is 6.9 [
96
]. The age at which particular skeletal
sites show increased incidence of fractures differs between the sexes, for example
the incidence of distal radius fractures in females increases markedly from the age
of 55, whereas in men the incidence of these fracture does not increase until after
the age of 75 [
96
].
In females, there is accelerated loss of bone mass from the onset of menopause,
which can be within the 5th decade but more usually in the 6th decade. Cessation
of estrogen production removes an important control on osteoclast activation,
Search WWH ::

Custom Search