Biomedical Engineering Reference
In-Depth Information
100
Before delivery of the T wave shock, synchronization is car-
ried out by an asynchronous burst V00 so that T wave timing
could be anticipated. According to a set coupling interval or
delay after the last synchronization pulse, a shock is deliv-
ered, the timing of which is assumed in the cardiac cycle vul-
nerable phase. T wave shock energy is set in the range 1-2 J.
PES allows the ICD to deliver an optional number of pac-
ing pulses in regular time intervals (S1) followed by prema-
ture stimuli (S2-Sx) inducing or terminating arrhythmias [74,
75]. Excitation pulses (or pulse S1) serve for management of
pacing and cardiac rhythm at a rate higher than the intrinsic
action. Thus, precise synchronization of the stimuli with the
cardiac cycle is ensured. The initial pulse S1 is coupled with
the last sensed or paced event by interval S1. Pulses are
applied gradually in asynchronous modes A00 or V00 accord-
ing to a programmed prescription until a pulse is encountered
that is set to off. The induction of PES is complete after an
excitation drive train and extra stimuli are applied and after
ICD detection is restored automatically. PES can be applied
to induce both atrial tachycardia and VT.
Burst induction is applied to induce or terminate arrhyth-
mias; it allows various types of pacing, possibly applied
asynchronously, either in an atrium or a ventricle. A burst
with optional cycle length, gradual acceleration, or set at
50 Hz, can be selected depending on the manufacturer and
the type of ICD.
Commanded (manual) therapies are started from the pro-
grammer. Available types include a defibrillation (cardiover-
sion) shock and all types of ATP. Commanded therapies may
be applied independent of programmed detection and ther-
apy parameters. If a device is applying a therapy and a com-
manded method is initiated, the electrophysiological function
has a higher priority and suspends the therapy or detection in
progress. The commanded shock function enables the deliv-
ery of a shock with adjustable energy and coupling interval.
The shock waveform and its polarity are identical to shocks
after the initial detection. Upon the delivery of the com-
manded shock, redetection is applied, and postshock pacing
is activated, if programmed. Commanded ATP also allows
the application of schemes independent of programmed
detection and therapy parameters [ 70, 77 ] . During electro-
physiologic testing, temporary pacing settings can be used to
secure a patient. This may also be applied during a patient's
routine follow-up for the evaluation of the efficacy of deliv-
ered treatment.
80
60
Defibrillation
success
[%]
Measured DFT
(lowest cardioversion
success)
40
Measured
energy
margin
20
0
E
MAX
Energy
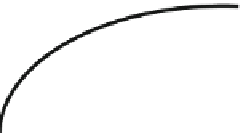
Fig. 10.7
Relationship between successful probability defibrillation
and shock energy
implanted device. The signal from the implanted lead should
be uninterrupted and without artifacts, similar to a surface
electrocardiogram. An interrupted signal may be a sign of
breakage or other damage to the lead or defective insulation.
To obtain acceptable lead signals, the configuration and posi-
tion of implanted leads must be evaluated for the suitability
for each patient and the sufficiency of programmed shock
energy or maximum energy shock for reliable tachycardia
cardioversion.
Testing a defibrillation threshold (DFT) allows a safety
reserve for a treatment shock to be determined. The safety
reserve is calculated as the maximum energy of the ICD
minus DFT, where DFT is the minimum tested energy that
reliably turns VF or polymorphic VT into a sequence of test
arrhythmias with descending defibrillation energy. DFT
refers to the energy level at which arrhythmia is last con-
verted (Fig.
10.7
). Such testing is carried out by inducing
arrhythmias using a programmer and by delivering shocks to
the patient's heart from the ICD via defibrillation shock elec-
trodes. During a shock or delivery of ATP, conducting objects
or devices must be prevented from making contact with the
system because the energy could be diverted, resulting in a
decrease in the amount of energy delivered to the patient and
subsequent possible damage to the implanted system. It is
important that the cardioversion should be carried out as
soon as possible after the arrhythmia is induced because lon-
ger-lasting tachycardia is more difficult to terminate.
Reliable conversion should be proved at a lower energy
level than the device's maximum shock energy. Technically,
it would be ideal to identify a real defibrillation threshold,
that is, the minimum amount of energy required to terminate
VF. Because repeated action represents a considerable load
for a patient, each shock must be regarded as proarrhyth-
mogenic, and, since the defibrillation threshold depends on
many circumstances, energy 10 J lower than the device's
maximum shock energy is often tested. Between induced
10.5.1 Determining the De fi brillation Threshold
After lead connectors are connected to the ICD and the
device is placed into an implantation pocket, electrograms as
well as lead signals must be evaluated in real time using the