Biomedical Engineering Reference
In-Depth Information
Maximum
PAV
SAV
offset
PAV
SAV
Minimum
PAV
Shorter of MTR
or MSR intervals
LRI
Hysteresis
Interval
PAV
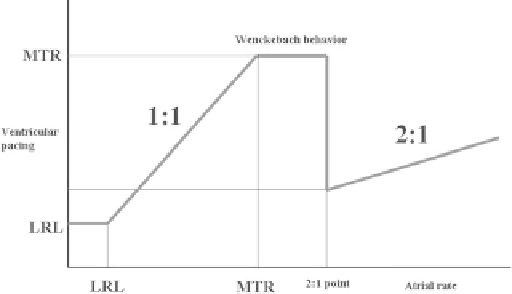
Fig. 9.13
Upper atrial rate behavior
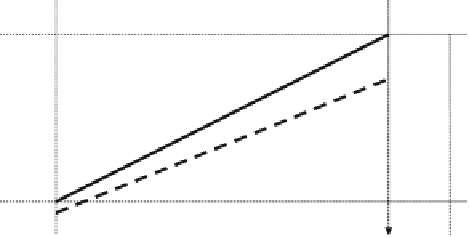
Fig. 9.11
Relationship between dynamic atrioventricular delay and
the lower rate limit [32] (© 2012 Boston Scientific Corporation or its
affiliates. All rights reserved. Used with permission of Boston Scientific
Corporation)
The maximum rate at which sensed atrial events are
tracked to ventricular pacing in a 1:1 ratio is determined by
the MTR parameter. The MTR applies to tracking pacing
modes, in particular to DDD(R) and VDD(R). The response
of the device at fast atrial action in these modes is determined
by the relationship between the TARP and the MTR or MSR
interval. The highest atrial action the device is capable of
tracking before a 2:1 block is determined by the relationship
60,000/TARP, where TARP = SAV + PVARP. The system does
not allow the programmed MTR interval to be shorter than
the TARP, and if the TARP is shorter than the interval corre-
sponding to the programmed MTR, the pacemaker reduces
the rate of ventricular pacing by Wenckebach behavior at the
MTR value. If certain algorithms for the prolongation of the
AVI are on, such behavior may occur at rates lower than
MTR. Figure
9.13
shows the procedure of tracking at increas-
ing atrial rate. The above-described pacemaker behavior is
referred to as upper rate behavior or upper rate response
.
As
Vp
As
Vp
EKG
AVI
PVARP
TARP
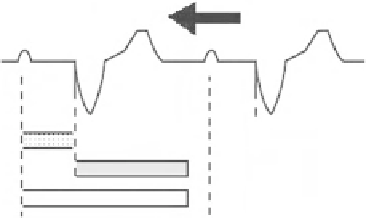
Fig. 9.12
Increasing atrial rate
If a sensed atrial rate is within the range of the pro-
grammed LRL and MTR values, ventricular pacing is deliv-
ered after the lapse of SAV or dynamic AV delay. All sensed
atrial activities are tracked to corresponding ventricular pac-
ing in the respective cardiac cycle. Nevertheless, if the atrial
rate increases (Fig.
9.12
), at certain rate, a P wave occurs in
the PVARP.
As a consequence, loss of conduction of certain atrial
events occurs as the device synchronizes ventricular pacing
with the sensed P wave. If the sensed atrial rate still increases
over the MTR, further atrial events will occur during PVARP.
These events are not tracked and do not trigger an AVI, and
the proportion of sequentially paced ventricular events to
sensed atrial events will decrease. This is referred to as
Wenckebach behavior. More P waves than paced QRS com-
plexes are identified on surface ECG. Upon acceleration of
the atrial rate, 5:4, 4:3, 3:2, to 2:1 blocks would gradually
occur. Finally, only every second sensed atrial event is
tracked; ventricular pacing is thus half the atrial rhythm. A
2:1 block can be desirable for the prevention of fast ventricu-
lar pacing at the onset of atrial tachycardia, but upon activity,
that is, upon physiological increase of atrial action, it is the
opposite, and the ventricular pacing may drop suddenly.
9.7
Automatically Switching Modes
If a device works in the VDD(R) or DDD(R) mode, tracked
atrial tachycardia may lead to fast ventricular pacing, which
is why the device must be capable of ceasing to track patho-
logically fast sinus rhythm to ventricles during episodes of
atrial tachycardia. This is made possible by an automatic
mode switching on the detection of fast atrial action. The
system's behavior when atrial tachycardia occurs is deter-
mined by the mode switch (MS) or atrial tachy response. If
detected atrial activity exceeds a set value, the MS switches
the pacing mode from a tracking mode to a nontracking mode
(e.g., from DDD(R) to DDI(R) or VDI(R); from VDD(R) to
VDI(R) or even VVI(R)). However, the modes with a sensor
are not commonly used for MS. Until the mode switches, the
ventricular pacing rate has the value of the MTR or shows
signs of a 2:1 block or Wenckebach behavior. The pacing
mode, to which the device is automatically switched to when
the MS condition is met, is referred to as a fallback mode.