Biomedical Engineering Reference
In-Depth Information
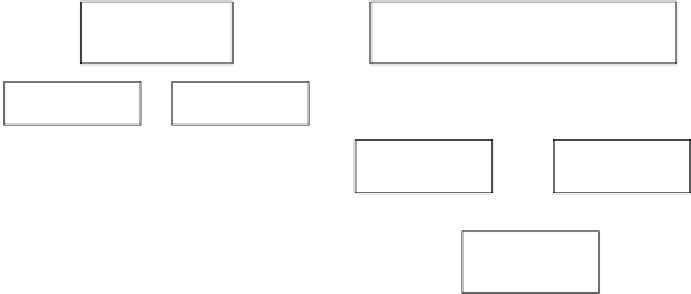
Pacemakers
PM
Implantable cardioverter-defibrillators
ICD
Single chamber
Dual chamber
With sensor
With sensor
Single chamber
VR
Dual chamber
DR
Without sensor
Without sensor
Biventricular
CRT-P
Biventricular
CRT-D
Fig. 2.1
Division of implantable cardiac devices
higher during sleep; it falls during the waking state and
decreases even more distinctly during physical exertion. The
pacing threshold is also influenced by pharmaceuticals: it
rises especially after the use of
I [A]
-blockers and class I antiar-
rhythmics but falls after corticosteroid use. Occasionally, a
brisk and inexplicable rise of the pacing threshold of some
patients can be observed. This is designated as an exit block.
b
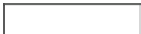
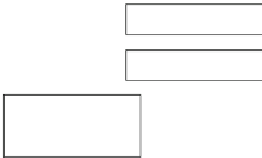
Rheobase
t [ms]
Chronaxy
2.3
Energy Sources and Longevity
of Implantable Devices
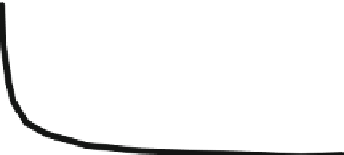
Fig. 2.2
Strength-duration curve
threshold can be expressed in terms of amplitude, pulse
width, or energy according to the direct proportion
E
A source of energy was always considered an important
problem of AIMDs. It is necessary to ensure reasonable ener-
getic capacity and reliability and to further their operational
performance of characteristics such as the voltage, self-dis-
charge current, energy density per volume unit, biological
compatibility, and structural shape. Historically, energy
sources can be divided into three groups: electrochemical,
radioisotopic, and biological sources. The electrochemical
(galvanic) cells comply best with the requirements stated
above, excluding the capacity. Their output voltage is not
dependent on the output, and they have a good structural
formability. At the end of the 1960s, radioisotopic thermo-
electric generators were applied. They had much better
energy capacity - they could operate for longer than 30 years.
However, a high price and possible danger of radioactive
substance leakage were disadvantages. Either biogalvanic
cells, which operate with body fluids such as electrolytes
during electrochemical reactions, or metal/oxygen biofuel
cells, in which the metal anode is consumed by oxidative
corrosion and the cathode decreases the oxygen present in
body fluids, have been used as biological or biochemical
power sources. However, undesirable reactions of the tissue
were observed in these cases. Electromechanical converters
can also be classified among biological sources, but they
required the patient's movement to make them work.
Nowadays, energy sources for implantable devices include
monocell and polycell lithium-iodine batteries. Voltage of
U
2
*
t
.
Cardiac pacing uses rectangular electric stimuli with pro-
grammable amplitude and width. Excitability of the heart
muscle can be expressed by parameters of a cardiac electric
stimulus that is able to activate cardiac depolarization, and
the so called Hoorweg-Weiss curve (strength-duration curve)
that expresses a relation between current amplitude and pulse
width of the pacing threshold is used for this (Fig.
2.2
). The
curve has the shape of hyperbola, and there are two charac-
teristic values that are defined on it:
Rheobase - a minimal pacing threshold current for the
»
•
theoretically infinite width of the pulse
Chronaxy - a pulse width at which the pacing threshold is
•
equal to twice the rheobase. In practice, within the
rheobase definition, the infinite width of the pulse is sub-
stituted by a definite one, for example 2.0 ms.
Either a doubled value of the voltage threshold or a tripled
value of the pacing threshold width is considered to be a safe
reserve of an electric stimulus output. The issue of the pacing
threshold is much more complicated and complex. The pac-
ing threshold is influenced by, for example, the type and mate-
rial of the lead used, by the distance between the electrodes,
and by the state of the tissue. The pacing threshold also
changes within the time after a lead implantation. However, a
considerable increase has not been observed yet, thanks to the
use of steroids. Within a daily cycle, the pacing threshold is