Biomedical Engineering Reference
In-Depth Information
270k
1k
4,7M
1h
1M
4,7m
47k
10 m
1k
4,7M
4,7M
10k
h82
5V
1M
37k
47k
10k
22k
12k
10k
10M
M1
4,7M
0,47m
1M
4,7M
270k
M68
1,8M
M1
2,3m
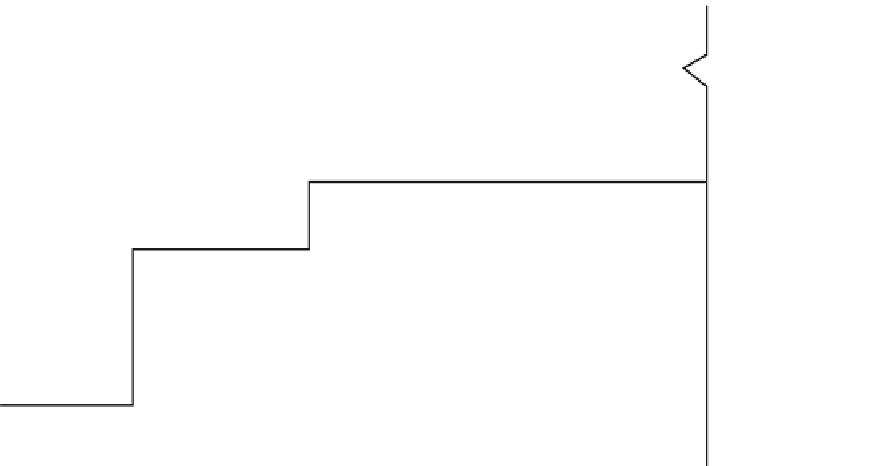
Fig. 1.3
On-demand pacemaker circuit (Used with permission of V. Bicik Research Institute for Medical Electronics and Modelling, Prague,
Czechoslovakia)
put into practice in 1983. In the mid-1980s, pacemakers capable
of adjusting pacing based on the patient's activity, sensed by a
piezoelectric crystal, were produced. In 1988, the possibility of
measuring intrathoracic impedance was introduced, allowing
controlled pacing according to a patient's physiological need
derived from the respiratory activity. In connection with the
development of new therapeutic and diagnostic methods, a new
revised five-position code was developed by the Intersociety
Commission on Heart Disease Resources. The original code
was augmented by the fourth (programmable functions) and
fi fth (antitachycardia functions) position. The fi ve-position
code used today, defined by the North American Society of
Pacing and Electrophysiology and the British Pacing and
Electrophysiology Group, was approved in 1984, modified in
1987, and further revised in 2002. Important improvements in
pacemaker technology are listed in Table
1.1
.
The development of implantable defibrillation technol-
ogy was triggered by the approval of a theoretical concept
in 1966. Three years later, an experimental laboratory
device was constructed, and the possibility of transvenous
defibrillation was tested. In 1975, the first experiment
was conducted on a dog. The first defibrillator was implanted
in a man in 1980. At first, the devices were implanted in a
subcutaneous pocket on the abdomen, and the epimyocar-
dial defibrillation lead was attached above the left ventricle
during open thoracotomy. The first implantable cardioverter-
defibrillators were equipped only with the function of a
shock sent upon the detection of ventricular fibrillation;
they lacked any diagnostic functions. The important
improvements in implantable cardioverter-defibrillator
technology are listed in Table
1.2
.
Fig. 1.4
Pacemaker Tesla LSK 201
The design of a preformed
J
-shaped atrial lead was an
important milestone because it facilitated the insertion and
fixation of the atrial lead, which had been rather difficult
before. In addition to the existing fixation options using
tines or a funnel, retractable screw-in active fixation also
was tested. Attention was given to the design of pacing
electrodes, the use of a rough fractal surface, and the decrease
of polarization voltages. Silicone rubber in the lead insula-
tion was replaced with polyurethane; as a consequence, the
insertion of two leads into one vein became easier.
The elution of a steroid by the fi rst lead to reduce in fl ammatory
response at the point of contact of the lead and the tissue was