Biomedical Engineering Reference
In-Depth Information
hyperkeratosis, hypogranulosis, and focal areas of downward
budding in the basal layer of the epidermis (49,51). Solar elas-
tosis is invariably present. Well-developed lesions may have
apoptotic cells, mitotic fi gures, involvement of adnexal struc-
tures, lichenoid infi ltrates, and a focal tendency toward
full-thickness involvement (Fig. 10.3). Full-thickness atypia
indicates transformation into SCC-in situ (51).
Treatment Rationale
Treatment Options for AKs
Given the premalignant potential of AKs, and the metastatic
potential of SCC, early treatment is paramount to preventing
disease progression. Treatment options for AKs depend on a
variety of factors, including severity of involvement, duration
or persistence of lesions, patient tolerability or desire for cos-
mesis, affordability/insurance coverage, and physician comfort
with available treatment modalities (49,58). Although AKs can
reliably be diagnosed by clinical examination alone (67), a low
threshold for biopsy should be exercised on atypical lesions, or
lesions not responsive to prior treatment.
Although singular or few lesions may be approached with
local surgical treatments, such as cryotherapy, curettage, exci-
sion, or dermabrasion, fi eld treatment may be more appropri-
ate when numerous lesions are identifi ed. In addition, fi eld
therapy will treat subclinical AKs. Chemical peels, laser resur-
facing, 5-fl uorouracil (5-FU), topical diclofenac, topical reti-
noids, and topical immunomodulators (imiquimod) are all
reasonable treatment options in addition to PDT.
A comparison of PDT to other fi eld treatment options for
AKs yields comparable clearance rates (68,69). In fact, a com-
parison of 100% clearance rates from phase III clinical trials
reported complete AK clearance with ALA-PDT of 72%, com-
parable to 5-FU (72%), and superior to imiquimod (49%) and
diclofenac (48%) (50). A direct comparison study by Kurwa
and coworkers (70) found comparable lesion area reduction
rates between ALA-PDT (73%) and 5-FU (70%).
Advantages/Disadvantages of ALA-PDT for AKs
Clearance rates of AKs following PDT has ranged from 68% to
98% (71,72). Assuming near equivalent or even superior clear-
ance rates of PDT compared with other fi eld treatment
options, PDT has several advantages in the treatment of AKs.
Improvement of photodamage, superior cosmesis, and better
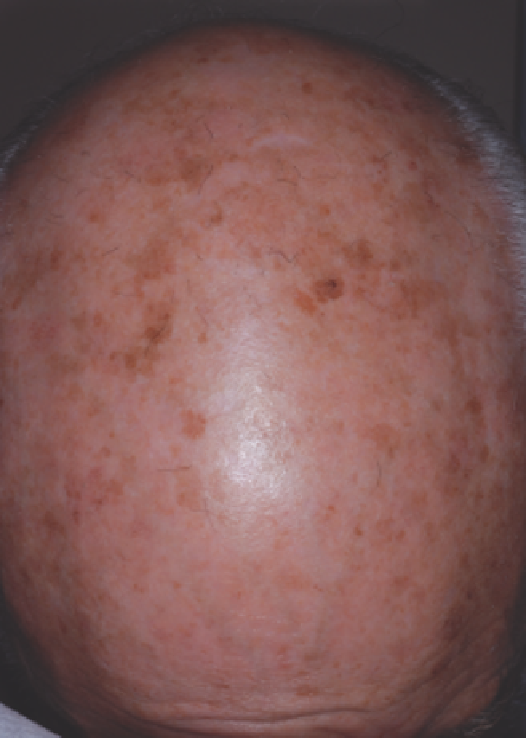
Figure 10.2
Frontal scalp of a 71-year-old white male demonstrating moderate-
to-severe photodamage. Numerous actinic keratoses characterized by erythem-
atous scaly slightly elevated plaques are visible on a background of extensive
solar lentigines.
(
A
)
(
B
)
Figure 10.3
(
A
) Histopathologic section of actinic keratosis stained with hematoxylin and eosin at 20× magnifi cation. Lesion is characterized by alternating ortho-
and hyperkeratosis with nuclear atypia and architectural disorder. Keratinocyte atypia approaches full-thickness in middle area of lesion. Note the gray, fragmented
nature of the papillary dermis representing extensive solar elastosis. (
B
) Actinic keratosis, lichenoid variant. A brisk lymphocytic infi ltrate in the papillary dermis
accompanies cytologic atypia of epidermal keratinocytes and marked architectural disorder. Numerous apoptotic cells are visible within the epidermis.
Source
:
Courtesy of Wenhua Liu, MD, Consolidated Pathology Consultants, Inc., Libertyville, Illinois, USA.