Biomedical Engineering Reference
In-Depth Information
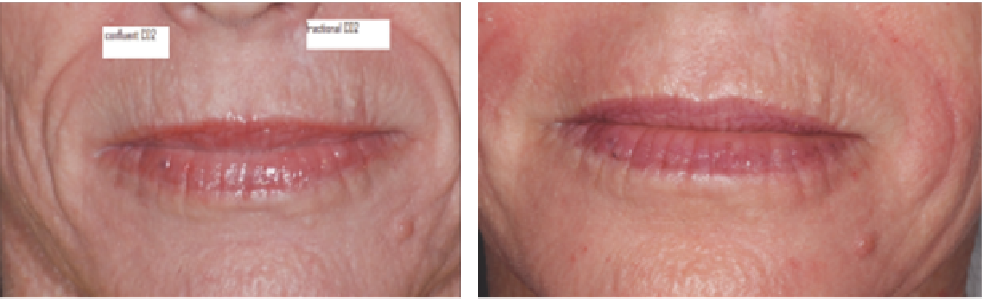
Fractional CO
2
Confluent CO
2
(
A
)
(
B
)
Figure 7.7
(
A
) Pretreatment perioral wrinkles. (
B
) Note greater improvement on confluent treated side.
Abbreviation
: CO
2
, carbon dioxide.
clinical considerations
Although ablative fractional lasers have an improved safety
profi le versus their nonfractional counterparts, excessive heat-
ing (too large a depth or density) can create scarring, dyspig-
mentation, and infection. Accordingly, the surgeon must be
familiar with the treatment device, the mechanisms underly-
ing the treatment, and the appropriate parameters for the
desired effects. It is also important that the patient's expecta-
tions are realistic, that they are tempered by the knowledge
and experience of the treating physician and that they under-
stand the inherent risks in undertaking such a procedure.
depths of injury. Typically injury depths 400
μ
m or greater
with CO
2
wounds and 200
m or greater with Er:YAG wounds
are associated with some intraoperative hemorrhage. Consid-
eration should be given to the administration of antiviral and
antibacterial prophylaxis. This is discussed in detail in the sec-
tion on “Complications” associated with ablative fractional
treatment.
μ
applications
There is an ever-expanding group of applications for fraction-
ated devices. Initial studies were focused on photoaging, includ-
ing dyspigmentation and rhytides (Fig. 7.8). However, more
recent investigations have revealed possible utility in other
arenas.
contraindications
Absolute contraindications to the procedure include a history of
keloid scarring (of the face). Relative contraindications include
a history of vitiligo and psoriasis (due to koebnerization), vas-
culitis, active skin infection in the area to be treated, use of oral
retinoid within 6 to 12 months prior to the procedure (21),
immunosuppression, and a history of radiation treatment to the
target area (15).
Photoaging
The fi rst studies using fractional devices were conducted by
Manstein et al. using a nonablative laser in 2004 (1). Since that
time, there have been many studies supporting the role of abla-
tive fractional devices in the reversal of photoaging. Specifi -
cally, dyspigmentation in the form of lentigines and seborrheic
keratoses, telangiectasia, and rhytides have all improved. The
greatest advantage of fractional lasers is the lower risk of infec-
tion and long-term hypopigmentation. In cases of microspot
ablative fractional remodeling, there have been no reports of
delayed hypopigmentation (at least in the absence of any scar-
ring or textural changes). On the other hand, fractional lasers
have not achieved as durable responses in wrinkle reduction in
the cheeks as traditional deeper CO
2
laser procedures (Fig. 7.9).
Also, without a same session tool that addresses pigment
(i.e., IPL, Q-switched laser), incomplete and only temporary
dyschromia reduction is observed. One advantage of fractional
lasers is the capacity for safety and effi cacy
off
the face (Fig. 7.10).
With the exception of very conservative confl uent CO
2
and
Er:YAG lasers (wounds confi ned to the upper half of the
epidermis), extrafacial rejuvenation shows an unfavorable
risk-to-benefi t ratio (22).
patient preparation
The patient must acknowledge indications, the expected ben-
efi ts, potential risks, complications, and adverse effects for the
procedure. Pre- and posttreatment clinical photos should be
taken and cataloged. Eye protection must be provided at all
times during the procedure. If working around the periocular
skin, metal corneal eye shields should be placed.
Analgesia may be provided by a number of methods. Most
patients can tolerate a mild to moderately aggressive treatment
with the use of topical anesthetic, local infi ltration, refrigerated
air, nerve blocks, tumescent anesthesia, or a combination thereof.
Oral anxiolytics can be of great benefi t. Patients having treat-
ment of the face should be advised to have a driver transport
them from the offi ce after the procedure. In situations where the
treatment will be very aggressive or the level of anxiety of the
patient prohibits safe execution of the procedure, consideration
can be given to conscious sedation or even general anesthesia.
Skin cooling before, during, and after the procedure can be
invaluable. The use of an air chiller can provide a signifi cant
reduction in procedure-related pain and should be available
for use.
Intraoperative hemorrhage is usually mild and transient,
particularly with CO
2
lasers, and is associated with increasing
Striae
Lee et al. treated 27 patients with white striae with a fractional
CO
2
laser. Pulse energy was 10 mJ and density was 10%. Only
one treatment was applied and improvement was assessed
3 months later. They found that about 60% of the participants
showed 50% or greater improvement in the appearance of the