Biomedical Engineering Reference
In-Depth Information
Published reports have correlated clinical signs with anatomic
depths of ablation (98). A pink color of tissue was found to cor-
relate with superfi cial papillary dermis, chamois-cloth appear-
ance for deeper papillary dermis, and waterlogged cotton-thread
appearance for reticular dermis. We have found this to be true,
but only in deep ablation, such as with treatment of plantar
warts or basal cell carcinoma of the back. When thinner layers
of ablation are used, as in resurfacing, these subtle clinical signs
are not seen. Unfortunately, a second report that has received a
tremendous amount of attention stated that color was an indi-
cation of depth of ablation: pink indicating epidermis, gray
indicating papillary dermis, and chamois yellow indicating
reticular dermis (99). These color changes are actually a misin-
terpretation of anatomic changes and not a reliable indicator of
tissue depth. If little residual thermal necrosis (less than 30
signifi cantly affect wound healing and result in a much deeper
wound than what is intended. Pulse stacking may occur inten-
tionally by concentrating repeated laser impacts on the same tis-
sue site or unintentionally by moving the handpiece at too slow
a pace or by using a CPG density that results in too much pulse
overlap (densities 7, 8, and 9) corresponding to 40%, 50%, and
60% overlap. This may be a signifi cant factor in causing scar-
ring, hypopigmentation, or poor wound healing (Fig. 6.7).
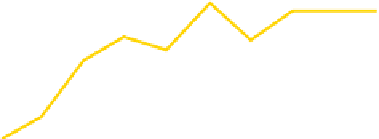
500 mJ/pulse at 1, 2, 3 pulses
Vaporization depth
300
1 pulse
250
3 pulses
2 pulses
m)
exists, thermal reaction will not be suffi cient to coagulate fi ne
papillary vessels, and the tissue will be pink because of the visi-
ble capillary blood fl ow. This is typical of the appearance of the
tissue after a single laser pass removing the epidermis. After a
second or third laser pass, the laser is reacting with the dermis
and leaves 70-100
μ
200
150
100
50
m of thermal necrosis, adequate for hemo-
stasis and resulting in whitish gray tissue. Further laser passes
tend to leave more thermal injury, resulting in progressive
yellow-brown discoloration, which is a sign of thermal injury,
not an indication of penetration into the reticular dermis.
These color changes probably do correlate to some degree
with depth of injury, but many inexperienced physicians have
interpreted this report too literally and spend much wasted
time attempting to recognize subtle color changes, when atten-
tion to the laser-tissue interaction with better comprehension
would be much more informative.
One study used posttreatment biopsies to compare three
pulsed CO
2
lasers with a CW CO
2
laser. After one, two, and
three passes, the depth of residual thermal damage measured
30, 80, and 150
μ
0
1
2
3
4
56789 0
Number of passes
Figure 6.5
With pulsed CO
2
laser ablation, using one, two, or three pulses per
impact site at 10 Hz, ablation plateau is reached in three to four passes, limit-
ing the ablation depth to approximately 250 μm.
500 mJ/pulse at 1, 2, 3 pulses
Thermal necrosis
350
300
3 pulses
250
2 pulses
μ
m, respectively, with the SilkTouch laser; 30,
200
100, and 150
μ
m with the SurgiPulse laser; and 20, 50, and
150
70
μ
m with the UltraPulse laser (80). The CW CO
2
laser left a
400-
m layer of thermal necrosis.
Although early studies appeared to show a relatively constant
amount of tissue to be ablated per pass (approximately 75
μ
100
1 pulse
50
m)
(79), it became clear in clinical use that a decreasing amount of
tissue was ablated per pass. To investigate this hypothesis, as well
as the effects of single-pulse vaporization versus multipulse
vaporization, or “pulse stacking”, and its possible relationship to
scarring, a study on excised tissue was done (100). Skin excised
for “face-lift” surgery was treated with one through ten passes,
wiping with saline between passes and using single-pulse, double-
pulse, and triple-pulse impacts at 10 Hz on the same impact site.
Biopsies were done to study the depth of ablation as well as
residual thermal necrosis. Be it a single, or double, or a triple
pulse used at either 250 mJ or 500 mJ per pulse, a similar curve
was generated showing that an ablation plateau was reached
after three or four passes at 225-250
μ
0
1
2
3
4
56789 0
Number of passes
Figure 6.6
When multiple pulses impact the same site at 10 Hz (double or
triple sets), a cumulative thermal effect occurs resulting in an increasing loss
of control of residual thermal necrosis. Single-tissue impacts, however, result
in excellent control of residual thermal damage, even after 10 laser passes.
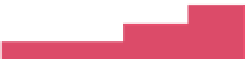
Average fluence (J/cm
2
)
Density
Overlap
1
2
3
4
5
6
7
8
9
-10%
0%
10%
20%
30%
35%
40%
50%
60%
2.4
3.0
3.7
4.6
6.0
7.0
8.2
11.9
18.5
3.3
4.0
4.9
6.2
8.1
9.4
11.0
15.8
24.7
4.1
4.9
6.1
7.7
10.1
11.7
13.7
19.8
30.9
4.9
5.9
7.3
9.3
12.1
14.0
16.5
23.7
37.0
6.5
7.9
9.8
12.3
16.1
18.7
21.9
31.6
49.4
8.2
9.9
12.2
15.4
20.2
23.4
27.4
39.5
61.7
m in the dermis (Fig. 6.5).
Residual thermal necrosis showed a linear relationship to both
pulse energy and number of passes, with single-pulse vaporiza-
tion gradually increasing to a maximum of 100
μ
m at pass no. 7.
However, pulse stacking had a marked impact on residual ther-
mal necrosis, because double pulses added signifi cantly more
thermal injury per pass and triple pulses even more per pass,
about 30
μ
Pulse energy
150 mJ 200 mJ
250 mJ
300 mJ
400 mJ 500 mJ
Figure 6.7
Most effective fl uences for treatment are 5-18 J/cm
2
, corresponding
to green and yellow zones of this chart. CPG settings of 9 can result in a fl u-
ence as high as 60 J/cm
2
.
μ
m (Fig. 6.6). This additional thermal injury may