Biomedical Engineering Reference
In-Depth Information
1
Introduction
In 1948, Albert Einstein was diagnosed with an abdominal aortic aneurysm (AAA),
i.e., his aorta had a permanent and irreversible localized dilatation having at least
a 50% increase in diameter compared with the normal one [
1
], Fig.
1
. Like him,
currently, it is estimated that more than 12 per 100,000 persons-year [
2
] are affected
by this relatively indolent but serious condition.
In an attempt to reinforce the aortic wall and delay the inevitable rupture that took
Einstein's life in 1955, Dr. Rudolph Nissen wrapped the visible anterior portion of
the aneurysm with polyethene cellophane. Nowadays, two more effective treatments
are available: open surgery and endovascular aneurysm repair (EVAR). While the
first is an invasive procedure, the second is a minimally invasive one whose main
advantages are decreased blood loss, less early morbidity and mortality, and shorter
hospitalization [
2
].
When EVAR was introduced, it revolutionized the treatment of aortic aneurysms.
However, and in spite of major advances in EVAR techniques, adverse reactions still
occur [
3
] and lifelong surveillance is recommended [
4
]. Due to these complications,
currently, questions are being raised regarding the follow-up costs [
5
] and alternative
approaches, such as a smart stent-graft, are being pursued.
A stent-graft is an endoprosthesis composed of a metallic scaffold and a
polymeric covering membrane. Its use and the technological background for the
development of a new device with sensing capabilities are described in this chapter.
After describing the current treatment options for aortic aneurysms, stent-graft
complications are presented as well as their surveillance techniques. Following, the
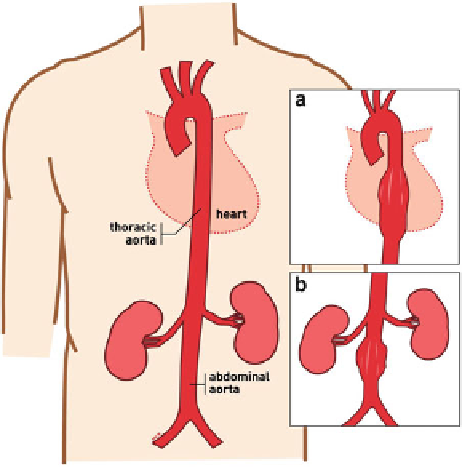
Fig. 1
Representation of a
normal aorta, (
a
) a thoracic
aortic aneurysm (TAA), and
(
b
) an abdominal aortic
aneurysm (AAA)