Biomedical Engineering Reference
In-Depth Information
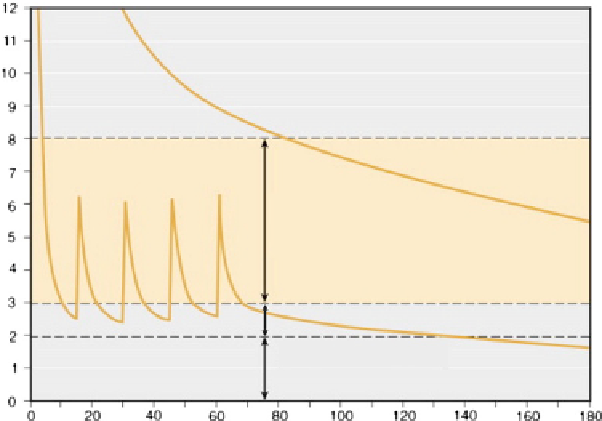
enough drug must be given in a bolus to ensure that the
animal remains nonresponsive to noxious stimuli for
a period of time; this leads to a “see-saw” effect with the
depth of anesthesia and physiological impairment being
maximal (and excessive) shortly after administration of the
drug and then gradually decreasing until the dose falls
below the theraputic range and the following dose is given
(
Figure 17.3
). If intermittent bolus administration is used
the resulting excessive physiological impairment can be
reduced by using boluses of a lower dose but higher
frequency. However, if possible it is advised that anesthesia
be maintained by continuous administration of anesthetic
drugs.
For a guide to drug doses see
Table 17.3
.
by other agents except for terminal (nonrecovery) proce-
dures such as perfusion-fixation, when the depressant
effects of this drug are considered unimportant. Thiopental
is a useful induction agent, but maintenance of anesthesia
by continued infusion or administration of successive doses
results in very prolonged recovery times, and it is better
replaced with propofol or alphaxalone.
Propofol
Propofol, an alkyl phenol, has been commonly used to
induce and maintain anesthesia in marmosets, macaques,
and chimpanzees (
Sainsbury et al., 1991; Ludlage and
Mansfield, 2003; Sleeman, 2007
). Its anesthetic effects
predominantly result from action on GABA
A
receptors. It
can cause transient apnea if given rapidly, but this can be
avoided by administering the initial dose slowly, over about
60 seconds. Some hypotension can occur following its
administration, but this is not generally a concern in healthy
individuals. The dose of propofol required to maintain
anesthesia can be reduced by concurrent administration of
opioids such as fentanyl, alfentanil, or remifentanil. This
balanced anesthetic technique can be used to provide pro-
longed periods of anesthesia, with a relatively mild degree
of cardiovascular depression. Respiratory depression is
often marked, however, so it is strongly advised that
animals are mechanically ventilated. At the end of the
period of anesthesia, respiratory depression caused by the
opioid can be reversed by administration of a mixed
agonist-antagonist opioid such as nalbuphine or buprenor-
phine. The advantage of this technique over the adminis-
tration of a full opioid antagonist is the retention of opioid
analgesia. The reversal of mu agonist opioids by mixed
agonist-antagonist or partial agonist opioids was first
established in humans (
Rifat 1972; Robertson and Laing
Injectable Anesthetics
A number of commonly-used anesthetic regimens are
described briefly below.
Ketamine Combinations
As previously stated, the same ketamine combinations that
are used for immobilization can also be used to facilitate
brief surgical procedures, either with repeat bolus dosing or
by continuous intravenous infusion. See also the section on
“Ketamine combinations” above for details.
Barbiturates
Pentobarbital, a barbituric acid derivative, has been used
extensively for anesthesia of nonhuman primates, but it
causes marked cardiovascular and respiratory depression
and its effects are cumulative. Recovery from pentobarbital
is prolonged and often associated with involuntary excite-
ment and prolonged ataxia. Pentobarbital is better replaced
FIGURE 17.3
Pharmacokinetic simulation of
a single large bolus of intravenous anesthetic agent
(upper curve) and a smaller bolus of the same agent
followed by intermittent boluses (lower cur-
ve). The single large bolus results in plasma drug
concentrations, and therefore physiological impair-
ment of the animal, far in excess of those required. The
intermittent bolus scheme results in plasma concen-
trations that periodically fall below the therapeutic
range. Ideally, the plasma drug concentrations should
be continuously within the therapeutic range, which
can best be accomplished with a continuous infusion of
intravenous agent or use of a volatile anesthetic agent.
(Adapted from
Glass et al., 2010
.)
Therapeutic range
Return of motor
reflex responses
Emergence from
anesthesia
Time (minutes)