Biomedical Engineering Reference
In-Depth Information
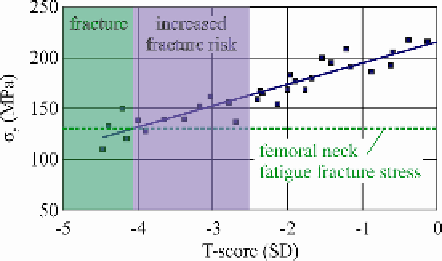
Fig. 7.
T-score as a fracture risk indicator
Even though DXA is a cost efficient BMD determinant, dominating the preference
of surgeons due to its simplicity, there are some limitations associated to the method
that may affect the accuracy of the introduced procedure.
As DXA quantifies the bone mass and not the bone quality of a specific site, mi-
cro-fractures in vertical trabeculae of cancellous bone will maintain undetected. It is
however widely accepted, that micro-fractures exert an important influence on the
mechanical strength of the bone. Despite this, DXA can be treated as a macroscopi-
cally indicator of bone strength. Especially in the hip region, where gait like loading
ensures constant remodeling and thus the probability of micro fractures is considered
as rather low.
Another possible limitation of our study is associated to the patients, the samples
were harvested from, as all of them were diagnosed with osteoarthritis. This might
have a twofold effect on the BMD-bone properties correlation.
Primary, it has not been established if the most common musculoskeletal disorders
of the elderly (osteoarthritisand osteoporosis) may be treated as independent, studies
have shown that the presence of one disease may act protective against the other
[43,44]. The effect however of this on the presented results, can be neglected as the
selected patients exhibited significant differences in terms of BMD.
Secondary, osteoarthritis has been associated to subchondral scleroses in femoral
head; the femoral neck and the trochander region however, are rarely affected by the
condition [45]. In order to circumvent this aspect, our methodology considered DXA
scans in femoral neck, trochanter and Ward's triangle and was determinedas reliable.
Additionally, osteoarthritic patients undergoing total hip arthroplasty were the only
group of patients from whom, we could receive bone samples from the femoral neck
region.
Studies have indicated that the femur carries a 30% of the applied loads in the sub-
capital region, while the base of the neck is subjected by 96% of the total load [46].
This strengthens the vital role of the femoral neck's capacity to transmit the compres-
sive stress from the joint to the shaft of the femur. Although the etiology of osteo-
porotic hip fracture is complex and multifactorial [47,48], bone quality is, without a
doubt, a major risk factor.
Search WWH ::

Custom Search