Biomedical Engineering Reference
In-Depth Information
300
200
100
0
0
2
4
6
8
10
12
14
16
18
20
22
24
26
28
30
32
34
Time (min)
b)
x 10
−8
c)
800
12
600
10
8
400
6
200
4
0
2
0
2
4
6
8
10 12 14 16 18 20 22 24 26 28 30 32 34
0
2
4
6
8
10 12 14 16 18 20 22 24 26 28 30 32 34
Time (min)
Time (min)
e)
6
x
10
−5
d)
120
5
100
4
80
60
3
40
2
20
0
2
4
6
8
10 12 14 16 18 20 22 24 26 28 30 32 34
0
2
4
6
8
10 12 14 16 18 20 22 24 26 28 30 32 34
Time (min)
Time (min)
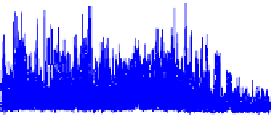
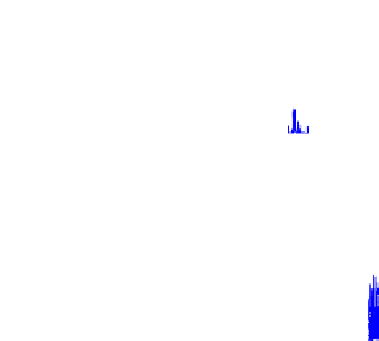
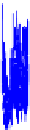
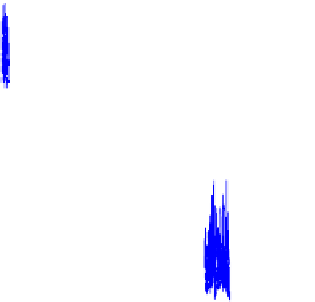
Fig. 3.
In vivo
validation results: a) Periflux 5000 results, b) CM results, c) AM results, d) M0
results and e) M1 results
microprobe: the slight increment verified after the nitrite injection and the abrupt de-
crease observed in consequence of the cardiac arrest. However, it should be remarked
that some lacks of correlation may occur given that the commercial probe and the pro-
totypes were located in different hemispheres, and blood flow changes can take place
with different extent.
4
Conclusions
Monte Carlo simulations used for the two new LDF prototypes validation showed re-
sults in accordance with the literature. For the non invasive prototype, the phantom
model presented here to evaluate the
in vitro
prototype response, has shown good agree-
ment with theoretical expectations. M1 increases with the scatterers concentration and
velocity, and with the fibre distances. The perfusion measured (estimated from M1)
also increases with the fibre distance and with the scatterers velocity, but only for the
aqueous milk solution of 25%. The mean depth increases with the fibre distance and
decreases with the milk concentration. The non linearities obtained in the measure-
ments leads us to built an acrylic phantom 1) with a plain surface easing the contact
probe/phantom and 2) with a higher volume of milk.













































































































































































Search WWH ::

Custom Search