Biomedical Engineering Reference
In-Depth Information
Pelvic Tilt
30
Ant.
20
10
Post.
0
Hip Flexion-Extension
45
Flex.
25
5
Ext.
−
15
Knee Flexion-Extension
70
Flex.
40
10
Ext.
−
20
Ankle Plantar-Dorsiflexion
30
Dors.
10
−
10
Plnt.
−
30
0 25 50 75 100
% Gait Cycle
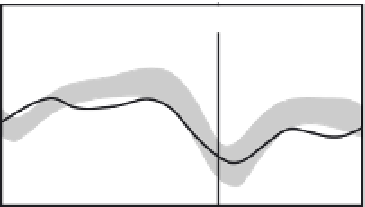
FIGURE 4.31
Sagittal plane kinematic data for the left side of a 9-year-old patient with cerebral palsy spastic
diplegia (solid curves). Shaded bands indicate
one standard deviation about the performance of children with
normal ambulation. Stance phase is 0-60 percent of the gait cycle, and swing phase is 60-100 percent, as indicated
by the vertical solid lines.
þ
/
palsy is a nonprogressive neuromuscular disorder that is caused by an injury to the brain
during or shortly after birth. The neural motor cortex is most often affected. In the ambula-
tory patient, this results in reduced control of the muscles required for balance and locomo-
tion, causing overactivity, inappropriately timed activity, and muscle spasticity. Treatment
options include physical therapy, bracing (orthoses), spasmolytic medications such as botuli-
num toxin and Baclofen, and orthopedic surgery and neurosurgery.
The sagittal plane kinematics for the left side of this patient (Figure 4.31) indicate signifi-
cant involvement of the hip and knee. Her knee is effectively “locked” in an excessively