Biomedical Engineering Reference
In-Depth Information
also MSCs. The potential advantages of using bone
marrow MSCs include low cell numbers required at the
initial culture, relative simple procedure for bone
marrow harvest, and the cell maintenance of high bi-
ological activity from older donors. However, the yield of
MSCs obtained from aspirated bone marrow blood is too
low (approximately 1 per 10
5
adherent stromal cells) to
use them as clinical cell source for tissue regeneration
and, therefore, an
ex vivo
cell expansion will be necessary.
The frequency of long-term repopulating cells is 1 in
35,000 total epidermal cells, or in the order of 1 in 10
4
basal epidermal cells, similar to that of hematopoietic
stem cells in the bone marrow
[26]
. Hematopoietic stem
cell frequency in the bone marrow was determined to be
1 in 10,000.
Stem cells have not taken on the identity of any spe-
cific cell type and are not yet committed to any dedicated
function; they can divide indefinitely and may be induced
to give rise to one or more specialized cell types. It seems
very likely that each tissue or organ has one somatic stem
cell even in adults. Awell-known somatic stem cell is the
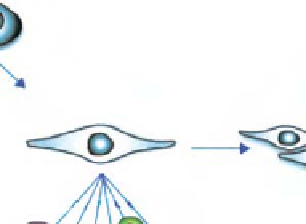
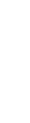
MSC that is able to differentiate into a variety of tissues
including skin, cartilage, bone, muscle, and fat, as illus-
trated in
Fig. 7.2-29 [27]
. It is clearly seen how versatile
this adult stem cell is for clinical application. Stem cells
of embryonic as well as adult tissue origin undergo the
differentiation process and eventually reach functional
maturity. In the use of stem cells as part of tissue engi-
neering, cellular behaviors including the differentiation
process must be carefully monitored.
Although the potential of ES cells is enormous, the use
of embryonal sources of stem cells is controversial and
major ethical and political issues impede their use. Issues
surrounding the rights of the unborn fetus, and sub-
sequent government regulation and limitations on avail-
ability and applicability of embryonic tissue, have put the
brakes on what appeared to be a rapidly approaching
clinical reality. In contrast, recent interest has emerged in
the use of bone marrow-derived stem cells for tissue
engineering applications. Adult-derived precursors po-
tentially provide ample quantities of an autologous
source of regenerative tissue without these ethical and
political issues. Although demonstrations of bone
marrow-derived MSC plasticity have been reported and
debated, widespread use of adult-derived tissue will
likely require a relatively painless, convenient, and safe
procurement method. Some have suggested that the skin
fulfills this role, while other reports have begun to
emerge suggesting that adipose tissue
d
which is elec-
tively aspirated in large quantities
provides a readily
available autologous source. Like bone marrow, adipose is
supported by a stroma whose isolation yields a significant
amount of cells capable of osteogenic, adipogenic, neu-
rogenic, myogenic, and chondrogenic differentiation.
d
Bone Marrow Cell (BMC)
Hematopoietic Stem Cells (HSC) Mesenchymal Stem Cells (MSC)
Self-renewal
Self-renewal
Commitment
Into commited lineage
Myoblast
Fusion
Endothelial
Progenitor cell
Osteoblast
Chondroblast
Neuroblast
Hepatoblast
Differentiation and Maturation
Osteocyte
Endothelial cell
Chondrocyte
Myocyte
Neural cell
Hepatocyte
Fig. 7.2-29 MSCs differentiation cascade. There are at least two types of stem cells in bone marrow, namely hematopoietic stem cells
and MSCs. One type of MSC repeats self-renewal, whereas the other type is committed to a specific cell lineage and goes through
a lineage process. MSCs are reported to differentiate into a variety of cellular types, such as osteocytes, chondrocytes, myocytes,
endothelial cells, neurons, hepatocytes, etc.