Biomedical Engineering Reference
In-Depth Information
HMEs are single-use, disposable units. They are
connected to the distal end of the breathing-circuit
tubing that is proximal to the endotracheal tube. Their
primary function is to maintain as much heat and hu-
midity as possible in the patient while preventing heat
and humidity from entering the absorber. HMEs are
occasionally known as ''artificial noses.''
Pressure versus volume-controlled
Historically, anesthesia ventilators have been relatively
simple, time-cycled, and volume-controlled which might
or might not meet the changing health care environment.
Patient care can be classified as acute or noncritical.
Acute care is a growing population at larger teaching
hospitals, as sicker patients are moved out of smaller
community hospitals by modern health management
organizations. This patient population is challenging to
manage and requires equipment that is more sophisti-
cated. Noncritical care machines should be simple to use,
with relatively little user-interface complexity.
One example of the limitations of traditionally sim-
plistic anesthesia ventilators is in the function of the bel-
lows pop-off valve. It closes completely during inspiration
so that FGF mixes directly with the set tidal volume
delivered. Changes in FGF will affect actual volume
delivered as a function of inspiratory time; the greater
the flow, the larger the tidal volume without making
any changes to settings. In response to the growing market
of acute care ventilated patients, manufactures have
begun to incorporate more complex pressure-support/
controlled ventilators into their anesthesia machines.
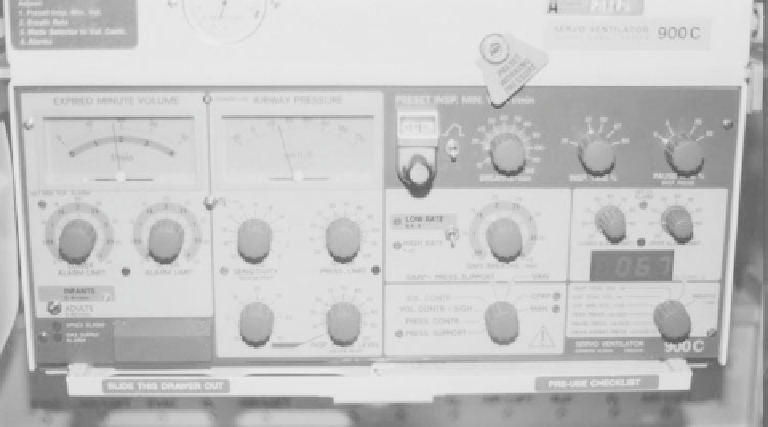
Ventilators
Ventilators (
Figure 4.4-5
) free the users' hands so they
are able to perform other tasks. It is a way to apply cy-
clical pressure to the equivalent of the breathing circuit
bag at a controlled rate and frequency. An expiratory
valve inside the ventilator closes during the inspiratory
cycle to direct drive gas into the bellows housing, creating
a positive pressure forcing breathing circuit gases to flow.
At the end of inspiratory cycle, the expiratory valve
opens, releasing drive gas from the bellows housing, and
returns the patient to atmospheric pressure. The working
gas that is used to drive the bellows varies by country, as
discussed previously. Comparable components between
manual and automatic ventilation are the bag and bellows
and APL and bellows pop-off valve. The bag and bellows
offer a means to buffer a volume as gases move in the
breathing circuit. The APL and bellows pop-off valves
control removal of excess gas from the breathing circuit
to the scavenging system, as discussed previously.
Both valves require a small amount of PEEP for prefer-
ential flow into the bellows (rather than the scavenger)
but the bellows pop-off is set a fraction higher, at about
2-3 cm H
2
O.
Airway pressure monitoring
Most volume-controlled ventilators are pressure-limited
and will not deliver settings if pressure limit is triggered.
Some have an adjustable pressure limit, and others are
preset. The transducer, which senses patient breathing-
circuit pressures, is physically located in the ventilator
fed from a tube taped into the breathing circuit. As
Figure 4.4-5 Siemens-Elema 900C ventilator.