Biomedical Engineering Reference
In-Depth Information
catheters are the most typical device used to aspirate
airways. Nasal-gastro tubes are used to empty stomach
contents that otherwise could interfere with the airway.
Probably the device with which most people are
familiar is a facemask. Masks are relatively simple devices
that come in numerous sizes, both disposable and reus-
able. They can leak if not fitted correctly, and they re-
quire a hand or strap to hold them in place. Their greatest
drawback is that they do not prevent possible aspiration
of stomach contents. They are not the best option for
longer cases, and excessive pressure can cause physical
injury to the patient.
To use most any other airway management tool
requires direct visualization with a laryngoscope. There
are standard airway classifications, depending on patient
anatomy. Laryngoscopes are available in various configura-
tions to best meet the needs of different airway anatomy.
Common blades that are used to obtain direct visuali-
zation of the vocal cords are straight, straight with
curved tip, or curved (Jackson-Wisconsin, Miller, and
MacIntosh, respectively). When patient anatomy or
trauma is such that use of a laryngoscope is difficult or
impossible, a fiber optic scope is used to help intubate
the patient. The two services that most often require
these tools are thoracic and plastic surgery. Thoracic
teams use them to visualize airways more easily, evaluate
tube placement, and aspirate secretions. Reconstructive
plastic surgery requires the use of fiber optic scopes, as
a significant percentage of these patients have disfigure-
ment or trauma that has altered normal anatomy. Video
equipment can help teach their proper use by enabling
two people to visualize the same image at once.
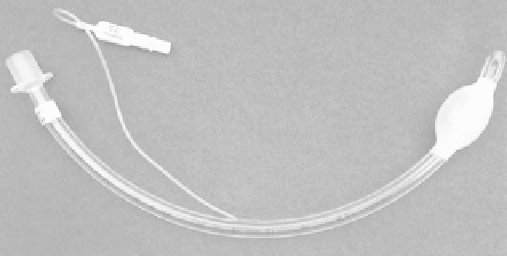
Endotracheal (ET) tubes are the most common item
used to maintain an airway. They are available in nu-
merous sizes and in cuffed (
Figure 4.4-1
) and uncuffed
configurations, although cuffed tubes are more common.
They have a balloon-like outer section at the distal tip
that inflates to seal with the inner walls of the trachea to
prevent leaks and inhalation of gastric contents or other
secretions. They are nearly always used on adults, and
they pose other potential problems if the patient is
intubated for periods over 48 hours. Uncuffed tubes do
not put pressure on the inside of the trachea that can be
more problematic with pediatric patients but can con-
tribute to airway leaks. The most frequent problem
associated with intubation is a sore throat from the
pressure exerted on the inner tracheal mucosa. There are
specialized ET tubes with two lumens used most fre-
quently during lung surgery, enabling ventilation of one
lung or both. Because they are in the immediate surgical
vicinity, these tubes are subject to greater external forces
and, therefore, are often reinforced. Another option is
the laryngeal mask airway (LMA). Because of its seal
design, its use is limited to ventilation pressures of about
20 cm H
2
O, and it does not prevent aspiration of gastric
contents. The LMA is most efficient in environments
where surgical procedures are generally short, and it is
a helpful tool for emergent needs.
Services that pose unique challenges are pediatrics and
oral surgery. Children are smaller, potentially making
tasks more challenging. In oral surgery, scavenging can be
challenging because surgery takes place in the immediate
area where gases are flowing.
Anesthesia machines
Anesthesia machines (see
Figure 4.4-2
) are constructed
of a number of systems assembled as one device. There
are standards developed by the American Society for
Testing and Materials (ASTM) (ASTM, 1989) for many
of the subassemblies used on or with the machines. Its
major systems can be broken down to gas delivery
(frequently referred to as the ''machine,'' itself),
vaporizer(s), breathing circuit, ventilator (including
related monitoring), physiological and CO
2
and agent
monitors. One standard does not cover all aspects of the
machine; for example, there are standards for machine,
ventilator, oxygen monitor, and breathing circuit.
Unfortunately, they can be vague and interpreted in
different ways, making them somewhat difficult to read
and understand.
Gas supplies
The machine's primary function is to reduce supply-line
pressures, mix a number of gases (most typically oxygen,
nitrous oxide, and air), and deliver a controlled output to
the breathing circuit. Primary gas supplies feed the
machine 50 psi. A pressure-relief valve opens above
75 psi in case of infrastructure system failure. Techni-
cians and engineers need to be familiar with a number of
pressure-measurement units. The most common are
pounds per square inch, millimeter of mercury, and
centimeters of water (psi, mmHg, and cmH
2
O, res-
pectively). A rough equivalent is that one psi is about 50
Figure 4.4-1 Cuffed endotracheal tube.