Biomedical Engineering Reference
In-Depth Information
H
I
u
I
RA
LA
aVL
H
III
u
III
H
II
m
u
II
I
u
H·m
lead vector
m
heart vector
H
LL
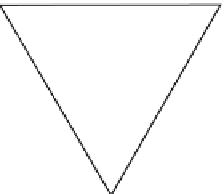
Figure 4.1-4 Einthoven's triangle. The triangle is in the frontal
plane of the patient. m is the heart vector bound to the ''center'' of
the heart; u is the instantaneous scalar voltage measured in a
respective lead;
a
is the instantaneous angle of the electric axis
of the heart.
-aVR
II
of the vector arrow describes a closed loop in the frontal
plane (
Fig. 4.1-5
).
The electrical axis of the heart can roughly be de-
termined by looking at the net area of a QRS complex. A
net positive area means that the heart vector has the
same direction as the lead vector. A small net area means
that the heart vector is perpendicular to the lead vector.
A negative net area means that the heart vector has the
opposite direction of the lead vector. It is interesting to
compare this interpretation which is based on a bound
heart vector with changing length and direction, with the
model which is a moving current dipole with constant
length and direction. With m and H
II
parallel the wave-
form will be monophasic, with m and H
III
perpendicular
the waveform will be biphasic.
The
dipole
model in ECG has been a hot topic.
2
Einthoven (1913) did not use the dipole concept, but
referred to the potential difference [V] between two
close points in the center of the heart. He thus defined
a current vector with the voltage difference between its
poles. There is an ambiguity here: A potential difference
may be regarded as a scalar [V], but may also be regarded
as an electric field [V/m] vector. A bipolar lead may be
regarded as an electric field transducer with scalar voltage
[V] output. Einthoven used the concept of electromotive
force (EMF) which may be considered to have direction
when related to the transducing mechanism of the force
exercised on a charge in an electric field, but may also be
regarded as a scalar potential [V]. So the heart dipole has
a vector moment [Am], the heart dipole moment has
a direction from plus pole to minus pole, the resulting
current density in the thorax is a vector field [A/m
2
], the
current density J and the electric field strength E are in
aVF
III
HR 52/minute
RR 1150ms
P 146ms
PR 234ms
QRS 92ms
QT 426ms
P axis 40°
QRS axis 24°
T axis 35°
P(II) 0.08mV
S (aVL)
−
1.12mV
R (aVF) 1.64mV
Figure 4.1-3 ECG waveforms of the six standard extremity leads
shown with the augmented leads interlaced between the bipolar
limb leads (Cabrera sequence).
obtained from the Einthoven triangle, and the heart vector
m [Am] is the unknown. The magnitude and direction of
m can be determined from measured potentials of at least
two leads (
Fig. 4.1-4
).
m represents a bound vector with the fixed origin in
the ''center'' of the heart, the lead vectors H are free
vectors. Sampling the
u
values of the leads I, II and III at
a given moment on
Fig. 4.1-4
defines the
instantaneous
value and direction (angle a in
Fig. 4.1-4
) of the heart
vector m. The mean direction during the QRS complex
defines the
electrical axis
of the heart. Mean direction is
used because the R tags are not completely concurrent
for the I, II and III leads. The electrical axes for the P,
QRS and T complexes have different directions (cf. the
text box of
Fig. 4.1-3
). During a QRS complex the locus
2
''Unfortunately, the application of the long known and well understood principles of potential theory to electrocardiography was not in general well
received. Many of the more or less theoretical and mathematical papers along these lines aroused a storm of opposition. Some of the criticism came
from physicians who felt that electrocardiography was a purely empiric science and that progress in the field could come only from comparison of
the electrographical findings with clinical and post mortem data. Much opposition came from physiologists, many eminent in their field, who not
only discounted any article of theoretical nature but also regarded the dipole hypothesis as rank heresy'' (Wilson, 1953).