Biology Reference
In-Depth Information
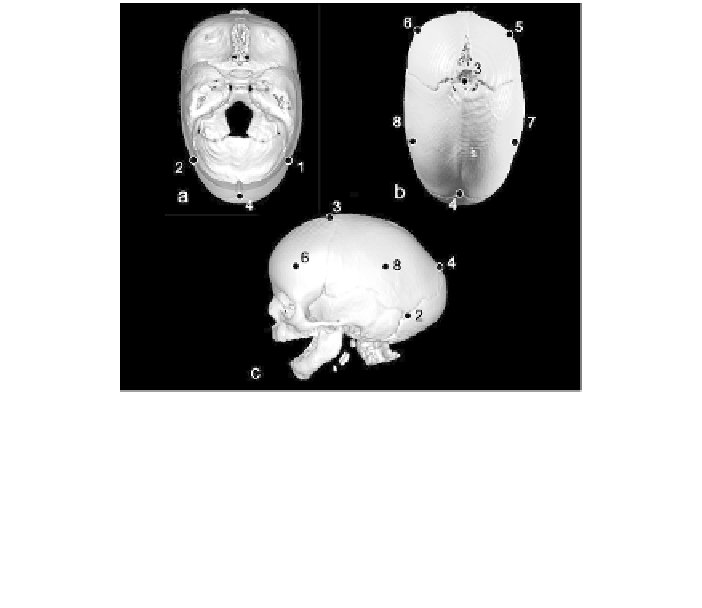
Figure 1.5
Three-dimensional reconstruction of a computed tomography (CT) scan of a
child with premature closure of the sagittal suture. Figure 1.5a shows a superior view of
the skull with superior surface of neurocranium removed. Figure 1.5b shows a superior
view of the skull with external surface of the neurocranium intact and demonstrating
approximate placement of the following landmarks: 3=bregma, 4=lambda, 5= right
frontal boss, 6= left frontal boss, 7= right parietal boss, 8=left parietal boss. Figure 1.5c
provides a lateral view of the left side of the skull with the following landmarks indicat-
ed: 2= left asterion, 3=bregma, 4=lambda, 6=left frontal boss, 8=left parietal boss.
mature closure of the sagittal suture. Isolated, or nonsyndromic synos-
tosis of the sagittal suture is fairly common (3 to 5 per 10,000 births),
occurring more frequently in males than in females (Cohen, 1986). The
developing neurocranium is made up of a number of roughly shell
shaped bony plates that align with one another at joints or articula-
tions called sutures. The sagittal suture lies between the paired pari-
etal bones (
Figure 1.4.a
). The anterior-most point of this suture lies at
the anterior fontanelle and in the more mature individual is defined by
the landmark bregma, which marks the intersection of the paired
frontal and paired parietal bones. The sagittal suture runs from the
anterior fontanelle (or the landmark bregma) between the two parietal
bones along the top of the skull until it intersects with the right and
left segments of the lambdoid sutures that separate the parietal bones
from the occipital bone. The intersection of the sagittal suture with the
lambdoid suture is marked by the landmark lambda. In most children,
the sagittal suture remains open until adulthood when it begins to
Search WWH ::

Custom Search