Travel Reference
In-Depth Information
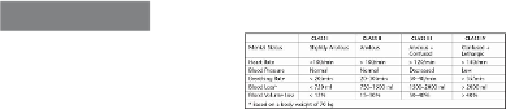
Table 3-2
Classification of Hemorrhagic Shock
Several initial management principles deserve emphasis. Treatment of hemorrhagic
shock begins with a complete examination of the injured person and quick assessment of
the circumstances of the inciting event. Optimally, the injured individual should be kept
on the ground where found until a spine injury can be excluded. Injured persons, however,
mayhavetobemovedexpeditiouslyfromthepotentialpathoffallingrockoranavalanche
for their safety as well as that of the rescue team. The first maneuver is to apply direct
pressure to external active bleeding sites. Extremity tourniquets, however, are rarely indic-
ated (
Chapter 12: Soft-Tissue Injuries
)
. The injured individual should be supine and, if un-
conscious, the airway should be assessed. If the individual manifests signs of hemorrhagic
shock, the feet should be elevated approximately 12 to 18 inches to empty venous blood
from the legs and maximize the circulating blood available to vital organs.
Ultimately, the successful management of severe hemorrhagic shock requires evacu-
ationfortreatmentatamedicalfacility.However,severaladditionalmeasuresmayenhance
the chance for survival. Hypothermia should be avoided, and body temperature must be
maintained. Wet clothing should be removed, and extra dry clothing from the rescue party,
sleeping bags, and blankets should be used to cover the injured person completely. An ex-
ternal heat source should be added in cold conditions because an individual in shock is un-
able to generate heat. Extremity fractures and dislocations should be immobilized to min-
imizeadditionalbloodloss.Pain,particularlyfromfracturedlargebones,maycompromise
the individual's physiologic compensation to shock and should be alleviated with narcotics
unless a severe head injury exists.
Intravenous administration of opiates is ideal because the onset is rapid and the dosage
can be titrated, but intramuscular injection is a reasonable alternative with the cautions that
the effects may be delayed and dosing must be more constrained. Supplemental oxygen
by mask should be added when it is available. Intravenous administration of saline is key
to restoring circulating blood volume outside the hospital and should be instituted when it
is available. Antibiotics should also be given if either an abdominal injury is suspected or
open soft-tissue wounds are present.
The timing of evacuation of an individual with overt hemorrhagic shock due to chest,
abdominal, and pelvic injuries is not straightforward. Clearly, immediate evacuation is ra-
tional if the distance to prompt air transport is relatively short. Conversely, a long overland
trek of a person with ongoing bleeding from a liver or spleen injury or a major pelvic frac-
ture may prove fatal, whereas maintaining the individual at the injury site to permit spon-
Search WWH ::

Custom Search