Travel Reference
In-Depth Information
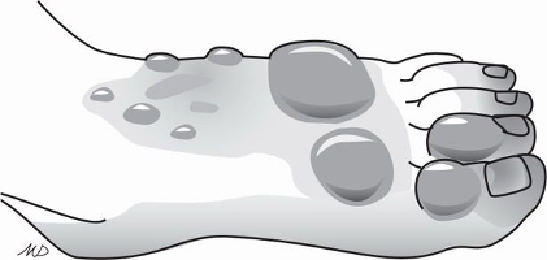
Figure 26-4. Frostbite of the feet manifested by blisters that do not reach the tips of the toes
After a week or ten days the dead frostbitten tissues develop a thick black covering
(eschar). Eventually, usually four to six weeks, the dead tissue, including entire fingers or
toes, separates spontaneously.
Treatment
The preferred treatment for frostbite is rapid rewarming in a water bath. However, op-
portunities for such therapy are rare because most frostbite injuries have thawed before the
individual arrives at a site where rewarming can be performed. Climbers or cross-country
skiers often have to be evacuated before they can be rewarmed. Thawing of the frostbit-
ten tissues during evacuation often is unavoidable. Individuals with urban frostbite, who
greatly outnumber those with wilderness frostbite, delay an average of twelve hours before
seeking medical care.
Rewarmingcanbestbecarriedoutinahospitalwherethepersoncanbekeptwarm,and
supplies forrewarming and later care are available. Treatment in a wilderness environment
should be attempted only when the following conditions can be met:
◆
The person does not need to use the frostbitten extremity until healing is complete.
Specifically, the person does not need to walk on a foot that has been frostbitten and
thawed.Thegreatestdamagefromfrostbiteoccurswhenfrozentissuesarethawedand
refrozen. Walking on a frozen foot produces far less damage.
◆
The person can be kept warm during rewarming and afterward for as long as recovery
requires.
If the person's body is cold, the blood vessels in his extremities are con-
stricted. Rewarming in such circumstances leaves badly injured tissues without an ad-
equate blood supply at the time it is most needed.
◆
Adequate facilities for prompt rewarming, including abundant supplies of warm water
and accurate methods for maintaining the temperature of the rewarming bath, are
available.
Search WWH ::

Custom Search